COVID-19 pandemic: the impact on Canada’s intensive care units
Abstract
The COVID-19 pandemic has exposed the precarious demand-capacity balance in Canadian hospitals, including critical care where there is an urgent need for trained health care professionals to dramatically increase ICU capacity.
The impact of the pandemic on ICUs varied significantly across the country with provinces that implemented public health measures later and relaxed them sooner being impacted more severely. Pediatric ICUs routinely admitted adult patients. Non-ICU areas were converted to ICUs and staff were redeployed from other essential service areas. Faced with a lack of critical care capacity, triage plans for ICU admission were developed and nearly implemented in some provinces.
Twenty eight percent of patients in Canadian ICUs who required mechanical ventilation died. Surviving patients have required prolonged ICU admission, hospitalization and extensive ongoing rehabilitation. Family members of patients were not permitted to visit, resulting in additional psychological stresses to patients, families, and healthcare teams. ICU professionals also experienced extreme psychological stresses from caring for such large numbers of critically ill patients, often in sub-standard conditions. This resulted in large numbers of health workers leaving their professions.
This pandemic is not yet over, and it is likely that new pandemics will follow. A review and recommendations for the future are provided.
Executive summary
The COVID-19 pandemic has challenged our ability to deliver life-saving acute and critical care to Canadians more than any other stress to the healthcare system in our recent history. It has exposed the precarious demand-capacity balance that has evolved in Canadian health care; one where capacity just matches demand during most periods of the year.
In its 2016 report on intensive care units (ICUs) in Canada, the Canadian Institute for Health Information (CIHI) found that ICUs had an average occupancy of 86 percent and 90 percent in large urban hospitals and teaching hospitals, respectively. This indicates that for significant periods of time, occupancy rates are nearly 100 percent, particularly at times of high demand such as during “influenza season” in the winter and during a busy “trauma season” in the spring and summer. High ICU occupancy rates, particularly those above 80 percent, have been shown to be associated with ICU mortality, hospital mortality, and ICU readmission within seven days of discharge. Based on this, it has generally been advised that ICUs should have an average occupancy of no more than 80 percent to be able to respond to surges in demand.
In addition to augmenting public health and acute health care capacity in Canada, this pandemic has shown us the need and value of cooperation across health systems. Without the regional and inter-provincial/territorial cooperation and transportation of critically ill patients that was undertaken, many more patients would have suffered or died from an inability to receive the care they needed. This is a demonstration of the ability and necessity to evolve our federally supported and provincially/territorially administered system of acute care to one that is more nationally connected and perhaps federally incentivized as a component of the transfer payment system.
It is also now clear that an effective health system response to a new illness demands the readiness to conduct the research needed to establish effective treatment on a national basis. The most efficient mechanism to quickly learn what does and does not work is to have a pre-existing national network of research infrastructure – investigators and research coordinators as part of a durably funded national acute and critical care network, conducting clinical trials, with pre-existing research ethics and contract agreements. National funders, regulators, research ethics boards, and researchers need to be ready to respond immediately to a declared public health crisis with input from patients, the population, and other stakeholders. In addition, involved stakeholders need to establish focused national observational and experimental research priorities that this network will turn its attention towards, focusing on sufficiently powered research designs that will definitively answer questions, as opposed to many individual and uncoordinated projects.
We have learned that pandemics have long-lasting effects on patients, health care workers, and the general population. An important element of this pandemic response should now be focused on preventing and treating post-COVID-19 syndrome in patients, supporting the mental and physical health of health care workers and solidifying the national research infrastructure needed to respond to the next health care crisis.
We must not forget what we have learned and continue to prepare for the next pandemic. In its 2004 report, The National Advisory Committee on SARS and Public Health found that there was much to learn from the outbreak of SARS in Canada - in large part because too many earlier lessons were ignored.
In 2006, Mr. Justice Archie Campbell, Chair of the SARS Commission wrote:
“SARS taught us lessons that can help us redeem our failures. If we do not learn the lessons to be taken from SARS, however, and if we do not make present governments fix the problems that remain, we will pay a terrible price in the face of future outbreaks of virulent disease”.
Canada needs to understand the impact of the COVID-19 pandemic on the country and to prepare for the next pandemic. As of 5 June 2022, this pandemic has caused the deaths of 41,354 Canadians over 26 months, a higher death rate than that seen in World War II in which 45,500 Canadians died over 5 and a half years. Viruses are jumping across species constantly and new outbreaks are likely to occur more frequently as humans increasingly encroach on other species’ habitats. Future pandemics caused by novel pathogens with case fatality rates higher than experienced with COVID-19 are not only likely but are inevitable.
High levels of immunity to COVID-19 must be maintained in the Canadian population
Although most people becoming sufficiently sick from COVID-19 to require hospitalization have been unvaccinated, fully vaccinated individuals represent 20 to 25 percent of hospitalizations and 10 to 12 percent of ICU admissions. These serious breakthrough infections are typically occurring in older individuals more than 6 months following their second vaccination shot. However, younger, apparently healthy fully immunized individuals are also contracting the infection, possibly due to a combination of decreasing levels of neutralizing antibodies over time and transmission from infected individuals with high viral loads and new variants. In Ontario, according to the Science Table, even with the omicron variant, unvaccinated people are currently almost six times more likely to be hospitalized, and almost 12 times more likely to require care in an ICU, than a person who has received two or three vaccines and booster shots. Put simply, the best way to prevent our ICUs becoming overwhelmed by COVID-19 infections again is to maintain a high level of immunity, including booster shots in the Canadian population.
Vaccination against a viral pathogen with such high prevalence globally is without precedent and we, therefore, have found ourselves in unchartered waters. However, as long as vaccines remain effective, a higher uptake of the vaccines will: (1) reduce the number of COVID-19-related deaths, (2) stem the spread of the transmissible strain of the virus, (3) reduce risk of other, potentially more, virulent strains evolving in the future, and (4) dramatically reduce the impact of the pandemic on our healthcare systems.
Without maintenance of immunity, Canadians and the health care system remain at risk. Public health officials and the medical profession must work to gain the trust of the population regarding the benefits of vaccination and work to increase the percentage of people who are fully immunized, recognizing that the definition of being fully immunized will evolve over time.
Canada’s ICU capacity must be expanded significantly
The ability to increase ICU capacity in response to a surge in critically ill patients is severely lacking and has been the case for some time in many provinces in Canada. Consequently, each province must consider how to increase the number of staffed ICU beds available for invasive mechanical ventilation and multiple organ support. In the first instance, this will require accurate regular reporting of the number of staffed, funded ICU beds available for the care of a critically ill patient requiring mechanical ventilation. Subsequently, funding will be required to expand existing ICUs and build new ones, as well as funding for the increased numbers of healthcare professionals needed to deliver critical care. This will require careful consideration at all levels of government and, likely, federal financial support. The eventual model would see an average occupancy in Canadian ICUs of no more than 80 percent, but with clear plans to rapidly increase ICU beds to 200 percent of regular occupancy in the event of a severe surge or another pandemic.
Since most ICUs in Canada operated at, or close to, 100 percent occupancy prior to the pandemic, an average increase of at least 20 percent in ICU beds over current capacity is necessary nationally, although some provinces will require a significantly higher percentage as their current ICU capacity is insufficient. One of the challenges is being able to allocate skilled human resources to other tasks when ICUs are less busy and being able to repatriate them when demand for critical care increases.
Critical care professionals must be retained, and new professionals recruited
New hospitals and ICUs are of little value without trained health professionals to work in them. Even prior to the pandemic, there was a shortage of nurses, including in ICUs. Critical care professionals have been warning of an impending workforce shortage, especially in ICUs, during the remainder of this pandemic and into the future. Because of the stress, ICU staff are struggling, many have already left their positions, and some are leaving the profession entirely. Unfortunately, it is likely that more professionals will leave in the coming months and years.
There has been extensive media coverage and concern expressed by professional associations about the physical, mental, and psychological impact of COVID-19 on the critical care workforce. Twenty-five months of constant exposure to suffering, death, and dying in understaffed, under-resourced, and often unsafe working environments have led to serious and potentially long-term negative consequences and strain on the health of critical care professionals including RNs, RTs, intensivists, and support staff.
Timely and easily accessible psychological services should be made available to the critical care staff since many have yet to process the traumatic experience they are currently living and have yet to unravel the extent of their emotional distress. This may have a significant impact on the retention of critical care staff at the end of this pandemic. It has been suggested that workplace violence, staffing shortages, and health care burnout are all connected.
An additional factor causing further moral distress in critical care staff is the inappropriate behaviour toward them by a vocal minority of patients, family members, and sections of the public. Critical care professionals are being exposed to verbal abuse that includes sexist and racist hate messages, as well as angry notes on their vehicles, death threats, baseless complaints, assault, anger, and mistrust, particularly during the fourth wave. These acts of violence are not only contributing to workers worsening mental, psychological, and physical health, but is putting their lives and safety at risk. The Canadian Medical Association and the Ontario Medical Association are calling for legislation to protect health care workers and patients from aggressive protestors.
The impact of this ongoing pandemic on the critical care workforce cannot be minimized. It is imperative that governments, hospitals, and health authorities implement strategies to train, retain and recruit this immensely valuable highly skilled workforce to ensure the delivery of quality care to Canadians that require care in our ICUs.
Canadian acute care hospitals must be upgraded
Many older hospitals in Canada struggled during waves of the pandemic to even provide an adequate and consistent supply of oxygen under the burden of the numbers of seriously and critically ill patients.
The heating, ventilation, and air conditioning (HVAC) systems in many older hospitals have not been upgraded to the current standard (12 air exchanges per hour) required when aerosol generating procedures are performed. When designing new hospitals, it is important to incorporate features that prevent airborne transmission of pathogens. Patients admitted for non-COVID-related illnesses were placed in rooms and open wards where they contracted the infection. Hospitals across Canada have reported significant numbers of outbreaks of hospital acquired COVID-19 infections that have resulted in illness and deaths of vulnerable patients and staff.
ICUs in many hospitals struggled with having to place two patients in cubicles built and equipped to care for one patient. It is time to examine the state of our acute care hospitals in Canada, consider how we can upgrade our hospital infrastructure to modern standards, where necessary, and to construct modern, state-of-the-art hospitals.
New hospital buildings must be acuity adaptable
As new hospitals and wings are planned and constructed across Canada, careful consideration should be given to incorporating acuity adaptability into the design and functionality of these new buildings. In particular, consideration should be given to supplying regular medical/surgical units with additional gas, suction, power, and data outlets so that they can be readily converted to the care of critically ill patients. In addition, these hospitals should have concealed gas, vacuum, power plumbing, and data outlets in non-clinical areas such as conference rooms, underground car parks, and even entrance hallways to enable those areas to become medical units in the event of a pandemic.
We must understand that SARS-CoV-2 is not finished with us
While it is widely hoped that the combination of immunization and natural infection is leading to the end of the pandemic, it is now clear this virus and future variants are not yet finished with us. The appearance of omicron and its many subvariants, make it clear that the virus has the capacity to mutate frequently and to create variants that have the potential to evade the immunity provided by our vaccines. Although fewer individuals infected with omicron have become seriously ill, this variant is so much more transmissible that hospital systems have been put under severe pressure. It has been widely stated that as viruses evolve, they tend to become more efficient at transmission and to also cause less serious illness after two years of dealing with COVID-19. However, the reality is that RNA viruses, such as SARS-CoV-2, mutate in a random fashion so there is no reason they cannot also cause more serious disease. In this respect, higher transmission rates increase the evolutionary potential of the virus by increasing the input of new mutations, potentially resulting in even more virulent strains.
In a best-case scenario, COVID-19 will become endemic. A pandemic is an emergency, with disease spreading out of control across countries and continents. “Endemic” suggests the infection is regular, present intermittently and predictable. However, if the pandemic stages fades and COVID-19 becomes endemic, it is critical that diagnostic testing capacity is not lost, that appropriate stores of personal protective equipment are maintained and that health systems remain capable of responding to new surges of the disease.
The federal and provincial governments must conduct honest and open in-depth reviews of their pandemic responses and initiate the development of a system of coordinated responses
The Canadian provinces have varied greatly with regards to when and how they implemented public health restrictions and vaccination mandates. Despite pleas from intensivists and public health experts, some provinces delayed the implementation of effective public health measures resulting in needless deaths and the eventual requirement to evacuate critically ill patients to hospitals in other provinces. Similarly, as COVID-19 cases surged in the early autumn of 2021, some provinces prematurely discontinued public health measures and ignored pleas from experts. Additionally, some provinces delayed the implementation of vaccine mandates and have been the first to remove them, as well as masking requirements. It is evident that it is unwise for jurisdictions to rely on vaccines alone, particularly when their rates of vaccination, including booster shots, is low. It is also apparent that the timing of initiation and removal of public health measures is vital to manage the severity of surges of severe illness due to COVID-19.
Despite messaging from some provinces, the pandemic is not yet over, and COVID-19 is not yet endemic. It is vital that each province and territory should perform an open and honest interim analysis of their individual responses and that the Government of Canada should conduct an interim review of the impact of the pandemic on health systems in the country to determine how to manage future waves of infection from yet unknown variants.
Formal mechanisms need to be developed to ensure consistency in public health responses, in line with acute hospital and critical care capacity across Canada. Additional mechanisms need to be developed to rapidly facilitate licensing requirements for health professionals being redeployed from one province to another. The Government of Canada must be prepared to enact the necessary emergency powers to protect its citizens, regardless of where they live, should the provinces not act appropriately if a new highly resistant variant develops.
The following is a list of other recommendations in the report
•
Accurate national data should be collected on the number of ICU beds capable of providing mechanical ventilation and other necessary supportive care to patients with multiple organ failure.
•
In addition to increasing ICU capacity and staffing, as recommended above, a selected group of non-ICU nurses in each hospital should be trained in critical care and be available if required. Their skills should be maintained by intermittent scheduled shifts in the ICU.
•
Although the pediatric ICUs (PICUs) provided substantial assistance to the care and outcomes of adults, it may be more efficient to maximize adult ICU capacity and to send staff to the adult ICUs rather than send adult patients to PICUs.
•
Strategies need to be implemented now to ensure appropriate use of adult and PICU resources during future crises.
•
Provincial licensing bodies should be prepared to rapidly provide licenses for intensivists and other ICU health professionals from other provinces and territories in the event of a surge in demand for ICU beds.
•
Health Canada, the Department of National Defence, and provincial departments of health should prepare contingency plans for the evacuation of critically ill patients to ICUs in other provinces in the event a province’s ICUs are being overwhelmed.
•
ICU Triage Plans should be standardized across all provinces and territories and the public should be made aware of their existence.
•
With appropriate precautions, family members and close friends should be able to visit patients in the ICU.
•
Increased funding should be allocated for the development and operation of specialized ICU Survivor Clinics. These would provide ongoing care in a holistic manner, including mental health issues, for patients with Post Intensive Care Syndrome.
•
Strategies should be implemented to actively monitor the well-being of the critical care staff to prevent moral and psychological distress, and to ensure that the impacts of workload changes are properly understood and mitigated where possible.
•
Mental Health Liaison Teams should be developed to facilitate and assist families navigating the system, and to ensure they receive appropriate mental health support in the community
•
Clinical research must be integrated into and across our health systems.
•
A discussion should be initiated on the lack of clinical research within Canadian health systems, and its consequences.
•
Clinical and biological data should be collected nationally for research purposes.
•
A standard trial contract agreement template should be available at research institutes across Canada
Introduction
This report reflects on the impacts COVID-19 has had and continues to have on intensive care services in Canada. It does not intend to provide an encyclopedic review of the science underpinning the care of patients with severe COVID-19, but rather aims to provide an overview for the public, those involved in health service administration, and provincial and federal public servants and politicians.
In a pandemic, the Federal Government is responsible for setting and administering national standards for the health care system through the Canada Health Act and providing funding support for provincial and territorial health care services. However, in Canada, delivery of health services is the responsibility of each province and territory, and they have organized and governed their healthcare delivery systems differently, depending on history, geography, population density, and local politics.
Population-level public health restrictions on travel and public gatherings have been implemented in many countries, including Canada, to slow virus transmission. Such restrictions have often been precipitated, in part, by the need to prevent or relieve pressure on hospitals and particularly on ICUs. In northern Italy, ICUs were overwhelmed at the start of the first wave of the pandemic. This resulted in increased deaths and the need to urgently develop and implement an ICU triage protocol (Faggioni et al. 2021).
Canada has one of the lowest numbers of acute care and staffed ICU hospital beds within the 38-member Organisation for Economic Co-operation and Development (OECD) countries. This has created a situation where the Canadian health care system has typically operated at or close to 100 percent capacity during waves of the pandemic. Consequently, in most provinces, wide-reaching public health restrictions and postponement of booked medical procedures were implemented to preserve the ability to deliver appropriate care to the large numbers of patients with severe COVID-19 related illnesses.
In this report we will attempt to answer several questions:
•
What is an ICU and how is it staffed?
•
What was the impact of COVID-19 on ICUs in Canada?
•
How could such a small proportion of critically ill COVID-19 patients overwhelm Canadian ICUs?
•
What is the course of illness and required treatment for critically ill patients with COVID-19?
•
What measures were employed by hospitals and health authorities to create extra ICU capacity?
•
What was the impact on pediatric ICUs?
•
What is the psychological impact on critical care professionals of working continuously under such severe pressures for 20 months?
•
What is the impact of an ICU admission on survivors and their family members?
•
What is “Canada’s Critical Care Research Agenda Related to COVID-19”, has it improved our healthcare systems’ response to the pandemic, and what does this pandemic teach us about research gaps?
•
How should Canada and its provinces respond to additional waves of COVID-19 and to future pandemics caused by novel pathogens?
History of ICUs
Harvey Cushing developed the first hospital area devoted to the care of patients following major neurosurgical procedures at the Peter Bent Brigham Hospital in Boston. This combined with surgical advances reduced the post-operative mortality dramatically from close to 90 percent to 8 percent. Cushing’s postoperative surgical ward only relied on meticulous and frequent clinical observation, having none of the monitoring and other equipment available in ICUs today. This approach was subsequently used to improve patient care and outcomes following major cardiac and thoracic surgery. However, the major advance came in 1952 during the massive polio outbreak in Denmark. The Blegdam Hospital in Copenhagen was overwhelmed by hundreds of mainly young patients, most of whom would die due to paralysis of their breathing muscles, unless artificially ventilated. There were not enough “iron lungs” to treat everyone, so patients were ventilated through a tracheostomy tube attached to a stiff rubber bag squeezed rhythmically by hundreds of volunteers. This approach was successful in saving thousands of lives in countries around the world, including Canada. Since then, critical care medicine has advanced considerably and become a specialty (Hollingham 2022; Kelly et al. 2014). Tens of thousands of Canadians who would otherwise have died have had their lives saved in ICUs across the country.
What is an intensive care unit and how is it staffed?
ICU staff and environment
Critical care is the level required by a profoundly ill patient who has a risk of dying without it. While critical care services may be temporarily provided anywhere in a hospital, after the initial stabilization of a patient they are usually provided in an ICU by specially trained professionals. Intensive care services are required to provide potentially life-saving therapies to the most seriously ill patients within acute care hospital settings.
The hallmarks of an ICU are the highly trained, multidisciplinary, inter-professional critical care staff and the use of specialized technology. The passion of ICU staff fuels an ethos of excellence that permeates the intensive care continuum. Critical care nurses have usually had experience in other hospital areas and 3-6 months of speciality-level education before commencing in the ICU. Foundational care for each patient in the ICU is provided by a bedside nurse, typically on a one-to-one basis. At the hospital and health system level, each ICU bed requires up to 5 critical care trained nurses to cover all shifts (typically 12 hours at a time), when considering time off and vacations. In addition, there are respiratory therapists, responsible for multiple patients, who assess, aid, and augment the patient’s breathing using specialized devices including mechanical ventilator.
Intensivists are physicians and surgeons who have typically completed 3-4 years of undergraduate education, 4 years of medical school, 3-4 years training in a base specialty (internist, pediatrician, anesthesiologist, emergency physician, or surgeon) before undertaking 2 years of critical care medicine residency training.
Other crucial and important allied health professionals providing patient care in an ICU include clinical pharmacists, occupational therapists, dieticians, speech-language pathologists, and social workers.
Beyond these health care professionals, patients in ICU often have a daily need for diagnostic imaging, blood and body fluid testing in clinical laboratories, and frequent consultation from additional medical and surgical specialists. In short, just as it is often said that a community is required to raise a child, it might also be said that an entire hospital is required to support and deliver essential intensive care services. While the challenges of providing excellent intensive care services may be concentrated within the walls of the intensive care unit, the resource implications of intensive care delivery systems are shared and felt across the entire hospital, and indeed health system.
Critically ill patients admitted to an ICU are surrounded by a large amount of sophisticated medical equipment (Table 1) used to continuously monitor, support, and manage the patient’s condition.
Table 1.
| Equipment | Purpose for use |
|---|---|
| Physiological monitors | To continuously display cardiac, respiratory, and neurologic status. |
| Infusion pumps | To accurately deliver specific concentrations of medications used to support blood pressure and sedation and to infuse other medications such as antibiotics, neuromuscular blockers, etc. |
| Point of care ultrasound | To evaluate cardiac function, guide central venous catheter insertion and assess status of lung parenchyma. |
| Mechanical ventilators | To support breathing and supply high concentrations of oxygen. |
| Hemodialysis machines | To remove excess fluid and toxins in patients with severe kidney injury. |
| Heart-lung bypass machines | To provide additional support for patients whose heart and or lungs are too sick for the other ICU therapies alone. This therapy is called extracorporeal lung support (ECLS) or extracorporeal membrane oxygenation (ECMO). |
Regionalization of advanced critical care services
All ICUs should be capable of providing care to a patient with lung injury requiring straightforward mechanical ventilation and blood pressure support using intravenous fluid resuscitation and vasopressors or inotropes. However, very critically ill patients may require more sophisticated and complex therapies such as various forms of renal replacement therapy, plasmapheresis, and extracorporeal lung support (ECLS), often available only in large tertiary care referral centres. Therefore, while COVID-19 has placed huge strains on the healthcare system as a whole and on the ICUs in particular, they were greater for ICUs in teaching and large urban hospitals that provide care for the sickest of the sick in Canada.
The critical care workforce
ICUs were created out of a need for a separate physical space where nurses would closely monitor and provide specialized and personalized care to injured, postoperative, and severely ill patients. With the advent of intensive therapies, single and multi-organ support devices, and critical care monitoring equipment, care has evolved into critical care medicine (Weil and Tang 2011; Scales, D. 2020) where a complex interconnected network of healthcare specialists and technology work in synchrony to achieve the best possible health outcome for critically ill patients (Scales 2020).
Departments of Critical Care within hospitals or health systems may be responsible for one or more ICUs and are typically led by a dyad of an experienced intensivist and a nursing director. Health professionals from professions other than nursing may also lead the non-medical component of these departments or ICUs.
Accessing recent Canadian data on the critical care workforce has proven to be a challenge; this is an issue of concern for pandemic and surge capacity planning. In the following sections, the information on the availability of the critical health human resource pool that was, and to some extent still is, the backbone of intensive care service as applied to COVID-19 is presented. COVID-19 has exposed the absence of accurate information on our intensive care workforce as a risk which needs to be addressed to improve Canada’s pandemic preparedness and response in the future.
Critical care nurses
Critical care nurses provide continuous bedside care for patients experiencing life-threatening illnesses. They are highly specialized nurses that use their expert knowledge, skills, and advanced problem-solving abilities to support these critically ill patients and their families throughout their ICU stay (Canadian Association of Critical Care Nurses 2017).
Even before the onset of COVID-19, many hospitals across the country struggled with understaffing and lack of trained critical care registered nurses. Coupled with the fact that many ICUs in Canada run at 90 to 100 percent capacity, there has been even greater pressure on the ability to provide the high level of care required in critical care during the current pandemic. In addition, the physical pressures of overwork and psychological trauma are driving ICU nurses from the profession in increasing numbers (see below).
In 2019 there were 20,084 identified critical care registered nurses (RNs) or nurse practitioners (NPs) in Canada. (Canadian Institute for Health Informatics (CIHI) 2021a, 2021b).
The last available registered nursing workforce profile report from the Canadian Nurses Association (CNA) dates to 2011 (Canadian Nurses Association 2019). This document provided the following demographic data, as seen in Table 2, specific to critical care:
Table 2.
| Profile description |
|---|
| The average age of a critical care nurse is 40.4 years. |
| 90.9% of critical care nurses are women |
| 63.4% work full-time, 28.5% work part-time, and the remaining work on a casual basis. |
| 94.4% of critical care nurses have a staff nurse position, whereas 1.7% are in a managerial position and 3.9% are in another position (not specified). |
| 56.7% of critical care nurses are Diploma prepared, 41.2% are Baccalaureate prepared, and 2% are Master’s prepared. |
There is great interprovincial variation in the duration, content, and mode of delivery for training and preparation of critical care nurses, and post-registration specialty programs can range from a 6-week hospital-based orientation to a 6-month critical care certification in a post-registration educational program (Gill et al. 2012; Rose et al. 2008). A higher ratio of registered nurses with a critical care qualification results in better patient outcomes, especially when coupled with specialty certification (Bloomer et al. 2019; Kendall et al. 2009).
The Canadian Nurses Association (CNA) provides specialty certification in both adult and pediatric critical care via a national examination. Specialty certification has been shown to positively affect patient outcomes including lowering mortality, complications, failure to rescue, falls, and healthcare-associated infections and increasing patient satisfaction. Nurses’ outcomes, such as greater knowledge/skills, empowerment, and job satisfaction were also positively affected, as well as organizational outcomes including a lower intent to leave, turnover and vacancies (Halm 2021; Coelho 2020; Conley 2019). According to the latest CIHI Nursing in Canada report (2021), there were 975 and 140 nurses certified, respectively, in adult and pediatric critical care in 2020. Since 2011, 12,141 nurses have been certified in adult critical care and 1,364 in pediatric critical care. However, there are no data showing the total number of Canadian critical care nurses who have a post-registration qualification in critical care nursing. As of this day, it is unclear how many of these certified nurses continue to practice in critical care.
Staffing models, as outlined in consensus guidelines for critical care, include one RN for every one to two patients, depending on a patient’s acuity (Chamberlain et al. 2018; Bloomer et al. 2019). Nurse-to-patient ratios are contextually based and should reflect variability in census and acuity (Canadian Association of Critical Care Nurses (CACCN) 2019). In this respect, health professionals providing care to COVID-19 patients had higher workloads due to the need for donning and doffing personal protective equipment but, in particular, because of the need to prone these patients with severe pneumonia, which takes at least 6 nurses to perform safely. In addition, patients receiving ECMO treatment have high nursing workloads.
Patient safety and critically ill patient outcomes are impacted by several factors including nurse-to-patient ratio and the education level of critical care nurses. Several studies have shown that when a nurse-to-patient ratio decreases (from a ratio of one nurse to one patient [1:1] to a ratio of one nurse to two or three patients [1:2 or 1:3]), patient safety is jeopardized, and patient outcomes can be negatively affected. For example, reduced critical care nurse staffing is associated with increased mortality rates and increased risks of hospital acquire infection, and may also be associated with increased hospital costs, lower family satisfaction, and lower nurse-perceived quality of care (Rae et al. 2021). The level of nursing education of critical care nurses has also been shown to impact patient outcomes (Aiken et al. 2014; Conley 2019).
The impact of COVID-19 for critical care nursing has been complex. Given the time required to train new critical care nurses and for them to develop their expertise, not all strategies to increase the capacity of critical care nursing are equally effective. Assuming that rapidly upskilling nurses from subacute practice areas is the primary solution for critical care nursing staff shortages is a dangerous one as it could negatively impact critically ill patients. Furthermore, it shows little recognition of the knowledge, skill and expertise critical care nurses require to care for this patient population (Wynne et al. 2021; Tomblin-Murphy et al. 2021). We recommend that future pandemic preparedness planning teams critically review different human resource management strategies, including the use of a team model of care, and evaluate their impact on patient safety, healthy work environments, and nurses’ well-being and job satisfaction.
Respiratory therapists
Respiratory therapists (RTs) are highly skilled health care professionals who assist physicians and nurses in the diagnosis, treatment, and care of patients with respiratory and cardiopulmonary disorders. They use their knowledge and skills to provide safe and high-quality care to those experiencing breathing difficulties in a variety of settings, including the neonatal, pediatric, and adult intensive care unit (Canadian Society of Respiratory 2021).
In 2019 there were 12,294 practicing RTs in Canada (CIHI 2019), with somewhat different profiles (Table 3).
Table 3.
| Profile description |
|---|
| 52% of respiratory therapists are 20-39 years old |
| 59% report area of practice being primary Critical Care |
| 51% of respiratory therapists have a Diploma level of education |
| 41% of respiratory therapists have a Baccalaureate Degree level of education |
RTs require a 3- or 4-year college diploma or university degree program in respiratory therapy, which includes clinical training at one of 23 nationally accredited programs. Unlike critical care nursing, RTs are generalists capable of working in all areas of practice, including critical care, without additional training.
Early in the pandemic, there was concern that there would not be enough ventilators due to increasing numbers of COVID-19 patients requiring ICU admission. In March and April 2020, the federal government added 30,000 new ventilators to national stockpiles (West 2021). However, by the third wave, it became clear that limited human resources were the largest barrier to providing care to critical care patients, as using a ventilator safely and effectively requires formal training and ongoing competency. Studies have shown that RT-driven care can lead to decreased ICU and hospital days (Harbrecht et al. 2009). Ventilation strategies and in turn ventilator modalities have become increasing more complex over the last few years. Acute respiratory distress syndrome (ARDS) patients have traditionally been amongst the most complex to ventilate, with their mortality directly linked to the ventilation strategy utilized (Pelosi et al. 2021). Critically ill COVID-19 patients ventilated in ICU were all presented with or developed ARDS, and this increased ARDS patient load has presented a never seen before challenge for the RT workforce. It required new and innovative strategies to avoid mechanical ventilation and to reduce the damage caused by mechanical ventilation.
The nationally accepted standard for workload for RTs in critical care is one for five patients on respiratory support (i.e., ventilation, non-invasive ventilation) (West et al. 2016). Investigations have demonstrated the effectiveness of RT-driven respiratory care in acute care (Harbrecht et al. 2009; Kollef et al. 2000).
During the pandemic in some ICUs in Canada, workload increased so that one RT provided care to 12 patients on respiratory support, and many were asked to take on additions roles and responsibilities that they would normally not undertake. To meet the needs, many RTs came out of retirement (West 2021) and, in some jurisdictions, RTs trained physicians without pulmonary or critical care backgrounds to help fill the workforce gap. This shortage of trained RTs will not be quickly resolved as there only about 550 graduates from programs in Canada each year.
Clinical perfusionists
Clinical perfusionists set up, operate, monitor, maintain, transport, wean, and discontinue mechanical devices used for circulatory support in patients undergoing certain surgeries or requiring additional circulatory support for cardiopulmonary illnesses. They are highly specialized, crucial healthcare professionals who mainly work with the wider cardiovascular surgical team in the operating room and in intensive care units, in both adult and pediatric settings. (Government of Canada 2016; University Health Network 2021)
There are 327 specialists certified with the Canadian Society of Clinical Perfusion (Canadian Society of Clinical Perfusionists, personal communication, August 2021).
Clinical perfusionists must complete a respiratory therapy or registered nursing program with a minimum of one year of work experience as a respiratory therapist. Alternatively, they may be a registered nurse with a college or university program in clinical perfusion, including clinical training (Government of Canada 2016). There are only three programs for the training of perfusionists in Canada: Michener Institute for Applied Health Sciences in Toronto, l’Université de Montréal, and the British Columbia Institute of Technology (University Health Network 2021).
The use of Extracorporeal Life Support (ECLS) has become common in a small number of Canadian tertiary care health centers equipped to offer this therapy to critically ill patients with severe COVID-19 related ARDS. Clinical perfusionists are active and essential members of the multidisciplinary team caring for patients being treated with ECLS (Parhar 2020).
Critical care physicians/intensivists
In 2019, there were 491 intensivists practicing in hospitals in Canada (Table 4). Intensivists typically complete university undergraduate and medical education, followed by postgraduate clinical training in a base specialty, sometimes a subspecialty, and finally a 2-year residency training in critical care medicine. They may specialise in recognizing and managing acutely ill adult patients with single or multiple organ system failure requiring ongoing monitoring and support, or with infants, children, and adolescents who have sustained, or are at risk of sustaining life threatening, single or multiple organ system failure due to disease or injury. (Canadian Medical Association 2019).
Table 4.
| Profile description |
|---|
| There are 491 intensivists in Canada (approximately 1.3 intensivists per100,000 population). |
| 68% of intensivists are aged between 35 and 44 years old. |
| 71% of intensivists are men, 29% are women. |
| 59% of intensivists work in an academic health sciences centre, with the remainder working in non-academic health sciences centre hospitals or in administration. |
As evidenced by the scarce amount of demographic information on the Canadian critical care workforce provided in this report, there is a need for more robust, accessible, and up-to-date data to ensure relevant evidence-informed surge planning and workforce mobility. In addition, these data would help support health organizations and associations in answering their professional and educational needs.
What was the impact of COVID-19 on ICUs in Canada?
A 2021 Canadian Institutes of Health Information (CIHI) report shows that from March 2020 to June 2021, there was a monthly increase of about 3,000 inpatient admissions for respiratory conditions, and a total of 14,000 additional patients in ICU compared with the pre-pandemic data (Fig. 1). This increase was not evenly distributed; each successive wave of COVID-19 saw a higher number of patients with respiratory conditions and put added pressure on hospitals for beds and specialized resources such as ICU beds and ventilators. By April 2021, 87 percent of respiratory admissions to the ICU were for COVID-19 infections. COVID-19 displaced most other common respiratory illnesses such as pneumonia and chronic obstructive pulmonary disease, illnesses that would normally require the same hospital resources. By wave 3 in the spring of 2021, the need for ICU care and mechanical ventilation for patients with respiratory distress had increased by approximately 400 percent compared to pre-pandemic (CIHI 2021a, 2021b).
Fig. 1.

Globally, the COVID-19 pandemic has placed enormous strains on hospitals, particularly on intensive care units and healthcare professionals. From the start of the pandemic in March 2020 until September 2021, the CIHI has detailed national information on 103,376 patients hospitalized in 9 provinces (Quebec data unavailable) and 3 territories: 23,751 patients had been admitted to ICU and 13,978 (58.9 percent) required mechanical ventilation. Twenty-eight percent of those admitted to an ICU died (Statistics Canada 2021) and as of 10 April 2022, 37,928 have died in Canada from COVID-19. In addition to the official death toll of COVID-19, it has been reported that, based on an analysis of excess deaths beyond expected during the pandemic, deaths due to COVID-19 may twice the official number reported. (Moriarty et al. 2021).
The national data on the number of patients with COVID-19 hospitalized and admitted to ICU per million population showed that the highest numbers were in prairie provinces (Fig. 2). The causes could include lower vaccination rates, as well as the delay in implementing and earlier removal of mitigation strategies by the public health agencies in these provinces compared with other parts of the country. Furthermore, these provinces have some of the lowest ICU capacities in Canada (see Fig. 3).
Fig 2.

Fig. 3.

How did such a small proportion of critically ill patients with COVID-19 overwhelm Canadian ICUs?
During a pandemic or major localized outbreak, public health measures such as masking, improving ventilation, hand sanitizing, physical distancing, and varying degrees of societal lockdown are used to reduce the spread of infection. The intensity of the measures may depend on the rate of infection and the impact on hospital, as well as the impact on the health system as a whole. (Institutes of Medicine 2007). The challenge of managing large numbers of patients critically ill with COVID-19 overwhelmed hospitals and ICUs during the waves of this pandemic. In turn, this influenced the timing and severity of the public health restrictions implemented at varying times provincially, nationally, and internationally.
In recent years, hospitals and provincial health authorities across Canada have worked hard to make acute care as efficient and lean as possible by reducing the numbers of acute care hospital beds and increasing care in the community. Consequently, Canada has one of the lowest numbers of acute care hospital beds in the 38 nation Organisation for Economic Co-operation and Development (OECD) (Fig. 3).
This explains why Canada currently has the highest acute care hospital bed occupancy of all countries in the OECD (Fig. 4). Taking an economic perspective to provide an efficient, lean care left Canadian hospitals in a precarious situation during the current pandemic as beds used to accommodate acutely ill COVID-19 patients displaced other patients who would otherwise be receiving care in those beds. High occupancy of curative (acute) care beds can be symptomatic of a health system under pressure. Some spare bed capacity is necessary to absorb unexpected surges in patients requiring hospitalisation. Although there is no consensus about the “optimal” occupancy, an average occupancy of 85 percent is often considered a maximum to reduce the risk of bed shortages (OECD 2021, National Institute for Care Excellence (NICE 2018).
Fig. 4.

Canada’s excessively lean acute hospital capacity has also contributed to the huge backlog of over 700,000 surgical procedures and an unknown number of diagnostic procedures, as hospital spaces and healthcare personnel were reallocated to the care of patients with COVID-19 (Government of Canada 2022a, 2022b).
Canada also has one of the lowest numbers of ICU beds on a population basis among several OECD countries (Fig. 5). Germany, with the highest number of ICU beds by population, was able to accept 113 ICU patients from Italy, France, and the Netherlands when the ICUs in those countries were overwhelmed (Fowler et al. 2015; McCarthy 2020; Statista 2021). The low ICU capacity across Canada (Table 2) was a major issue that led provincial governments to enact public health measures including stay-at-home orders and school closures in waves 2 and 3 of the pandemic (Detsky and Bogoch 2021).
Fig. 5.

Prior to the pandemic, most large ICUs in Canada frequently operated at close to or above 100 percent occupancy. High ICU occupancy, particularly above 80 percent, have been associated with increased ICU mortality, hospital mortality and ICU readmission within seven days of discharge (Chrusch et al. 2009). Postponements of booked surgical cases were frequent, particularly during surges in winter respiratory illnesses.
Table 5 is based on data from Fowler et al. (2015) and from the Canadian Institute of Health Informatics (CIHI 2020). Fowler at al defined an ICU bed as one that can provide care to a ventilated patient. This data was reported by intensivist leaders in each province. CIHI defines an ICU bed as one that a hospital or provincial health authorities considers a monitored bed for neonates, children, and adults, regardless of whether it is funded, staffed or capable of providing care to a ventilated patient.
Table 5.
| Fowler 2015 | Fowler 2015 | CIHI 2018-19 | CIHI 2018-19 | ||
|---|---|---|---|---|---|
| Population | ICU ventilator capable beds | ICU ventilator capable beds/100,00 population | ICU beds (CIHI) | ICU beds/100,000 population | |
| BC | 5,145,851 | 304 | 5.91 | 478 | 9.29 |
| AB | 4,428,112 | 292 | 6.59 | 400 | 9.03 |
| SK | 1,177,884 | 108 | 9.17 | 107 | 9.08 |
| MB | 1,379,584 | 93 | 6.74 | 165 | 11.96 |
| ON | 14,733,119 | 1122 | 7.62 | 1751 | 11.88 |
| QC | 8,575,779 | 885 | 10.32 | 1216 | 14.18 |
| NB | 781,315 | 103 | 13.18 | 144 | 18.43 |
| PE | 159,713 | 18 | 11.27 | 24 | 15.03 |
| NS | 979,115 | 141 | 14.40 | 128 | 13.07 |
| NL | 520,998 | 98 | 18.81 | 96 | 18.43 |
| NT | 45,740 | 6 | 13.12 | 4 | 8.75 |
| NU | 39,285 | 0 | 0.00 | 0 | 0.00 |
| YT | 42,176 | 0 | 0.00 | 0 | 0.00 |
| TOTAL | 38,008,671 | 3170 | 8.34 | 4513 | 11.87 |
CIHI provides regular online data updates on hospital facilities including ICU beds, but intensivists believe 2018-2019 data over-estimated the numbers for some provinces. Specifically, the numbers do not appear to be limited to funded and staffed beds capable of managing a critically ill patient requiring mechanical ventilation. For example, during the pandemic, Alberta Health Services publicly stated they had a total of 253 ICU beds. Similarly, media statements and contacts with intensivists indicate that Saskatchewan has 79 ICU beds. This suggests that data provided to CIHI includes unfunded, unstaffed ICU beds or that intermediate care/high dependency unit beds not staffed or equipped for providing care to mechanically ventilated critically ill patients are being counted.
There appears to be a reluctance or inability of the health ministries of some provinces to make accurate information on ICU capacity openly available in a timely manner. In contrast, a recently published report from the Ontario COVID-19 Science Advisory Table indicates that, just prior to the start of the pandemic, Ontario had increased its ICU bed capacity to 2012 staffed, funded beds. (Barret et al. 2021). There is an unmet need in Canada for transparent, accurate, and up-to-date information on staffed ICU beds capable of providing invasive mechanical ventilation in each province and territory.
Recommendation
Accurate data must be collected and published by CIHI on ICU beds across Canada capable of providing mechanical ventilation and other necessary supportive care to patients with multiple organ failure.
There are marked interprovincial variations in ICU capacity (Fig. 6) with the four most western provinces, where over 30 percent of the Canadian population reside, having an ICU capacity lower than most developed countries. (Table 5). Furthermore, while Manitoba, Saskatchewan, and Alberta have lower than average ICU capacity, they had the highest incidences of hospitalization and ICU admission. (Fig. 2.)
Fig. 6.

The limited number of specialist ICU beds in those provinces makes the health systems particularly susceptible to being overwhelmed by surges of infections during a pandemic, unless strict public health restrictions are put in place in a timely manner. The ICUs in Manitoba were seriously overwhelmed in wave 3, as were those in Alberta and Saskatchewan during wave 4, because the implementation of public health restrictions and vaccination mandates were delayed.
Recommendation: Canada’s baseline ICU capacity must be expanded significantly with additional surge capacity also built in.
The ability to increase ICU capacity in response to a surge in critically ill patients is severely lacking and has been for some time in many provinces in Canada. Each province must consider how to increase the number of staffed ICU beds capable of providing invasive mechanical ventilation and multiple organ support. In the first instance, this will require accurate regular reporting of the number of staffed, funded ICU beds capable of providing care to a critically ill mechanically ventilated patient. Subsequently, funding will be required to expand existing ICUs and build new ones, as well as funding for the increased numbers of healthcare professionals required to deliver critical care. This will require careful consideration at all levels of government, and likely, federal financial support. The eventual model would see an average occupancy in Canadian ICUs of no more than 80 percent, but with clear plans to rapidly increase ICU beds to 200 percent of regular occupancy in the event of a severe surge or another pandemic. In this respect, it is notable that Alberta has announced it plans to provide an additional staffed 50 beds over the next 3 years. (Bennett 2022).
Since most ICUs in Canada have operated at or close to 100 percent occupancy prior to the pandemic, this would suggest an average increase in ICU beds over current capacity of at least 20 percent is necessary on a national basis, but some provinces will require a significantly higher percentage increase as their current ICU capacity is insufficient. One of the challenges is to be able to allocate skilled human resources to other tasks when ICUs are less busy and to be able for them to return to the ICU again when demand for critical care increases.
What has been the cost of providing care to critically ill patients with COVID-19 in Canada’s ICUs?
CIHI has reported that the average cost of treating a COVID-19 patient in Canada (excluding Quebec) on a non-ICU COVID ward exceeded $23,000, four times more than a patient hospitalised with influenza. However, for a patient critically ill from COVID-19 requiring intensive care was estimated at more than $50,000, compared with $8,400 for someone who had a heart attack. (CIHI 2021a, 2021b)
What is the course of illness and required treatment for critically ill patients with COVID-19?
COVID-19 critical illness - clinical features and supportive care
For the past two years, through an extraordinary international effort, the extent and depth of knowledge about COVID-19 as a disease has increased dramatically. While much has been learned, more knowledge is still required as viral illnesses are often pathophysiologically complex, making outbreaks and pandemics difficult to predict.
There is substantial variability in the impact of COVID-19, ranging from asymptomatic infection to death. There is now extensive literature on risk factors associated with the development of severe disease and death, including age, sex, severe obesity, multiple comorbidities, and other conditions causing immunosuppressed state such as pregnancy and cancers. (Booth et al. 2021; Elkrief et al. 2020)
The most common reason for COVID-19 patients requiring admission to hospital is viral pneumonia, which causes progressive difficulty in breathing and a dangerous decrease in arterial blood oxygen levels. Surprisingly, some patients with pneumonia caused by COVID-19 are unaware they have dangerously low oxygen levels (Tobin et al. 2020; Wilkerson et al. 2020), prior to having difficulty breathing and leave it too late before seeking medical attention.
Initially, patients with severe COVID-19 pneumonia are usually provided oxygen at flow rates that can be supplied via piped-in oxygen from wall-based delivery devices available in most parts of the hospital. However, patients with severely low levels of oxygen saturation require higher flow oxygen therapy using special delivery devices. The need for high oxygen flow systems has placed some older hospitals under strain to meet demands when dealing with large numbers of COVID-19 patients (Rieger 2021; McGillivary et al. 2021). In some parts of the world – as reported in India during 2021 - some hospitals ran out of oxygen entirely, resulting in critically ill patients dying (Pearson 2020; McGillivary et al. 2021). Prior to the pandemic, high flow oxygen therapy was typically delivered to adults in ICUs but this has now become common on many non-ICU COVID medical units.
Mechanical ventilation
Patients whose oxygen levels cannot be maintained at or close to normal levels, or those with severe breathing difficulties, are given a combination of sedatives and pain medications then have a breathing tube attached to mechanical ventilator inserted into their trachea to inflates the lungs under pressure with a gas mixture of oxygen and air. Sicker patients, such as those with inflamed and stiff lungs or who cannot settle with sedation alone, often require the use of neuromuscular blocking drugs. These paralyze all the patient’s muscles so the ventilator completely controls the movement of the lungs, chest, and abdomen to maximize oxygenation and ventilation as safely as possible. While there was considerable discussion in the early weeks of the pandemic regarding possible shortages of ventilators, thankfully, there have been adequate supplies of modern ventilators in Canada during all surges to date. Sadly, this was not the case in India where the numbers of critically ill patients with the delta variant resulted in many hospitals running out of oxygen and ventilators and resulting in deaths (Baheti and Nayak 2022).
Patients requiring ventilation due to low blood oxygen levels are usually placed in the prone position (face and belly down) for up to 16 hours per day for multiple days, as this helps open the alveoli (air sacs) in the lungs. However, to prone a critically ill patient safely requires a team of at least 6 trained ICU staff, including at least one doctor capable of reintubating should the endotracheal tube become dislodged.
Extracorporeal lung support
If the patient’s gas exchange continues to deteriorate despite ventilation, consideration can be given to initiation of extracorporeal lung support (ECLS), which provides additional gas exchange by circulating blood through an artificial lung membrane allowing the damaged lungs to be ventilated at much lower pressures (Fitzsimmons 2022). This is a resource-intensive therapy requiring an experienced multidisciplinary team with training in initiation, maintenance, and discontinuation of ECLS in critically ill patients. Competent planning, resource allocation, and infection control are necessary to assure that ECLS is appropriately used during the COVID-19 pandemic. In institutions already near capacity due to hospitalization of COVID-19 patients, and patients with other conditions, use of ECLS for even a limited number of patients may overwhelm the institution.
Despite the technical and human resource demands involved, a systematic review of ECLS use in 1,892 COVID-19 patients across 22 studies, showed a mortality of 37.1 percent, similar to its use in other conditions that cause severe acute respiratory distress syndrome. This is remarkable as only patients with ARDS who have a projected mortality of nearly 100 percent with usual ventilator support are treated with ECLS. Younger patients and those with disease limited to the lungs tend to have better outcomes than older patients and those with multi-system dysfunction (Ramanathan et al. 2021). Barbaro et al. (2021) used the Extracorporeal Life Support Organization’s Registry to examine the outcomes in 4,812 patients with COVID-19 who received ECLS across 349 centres in 41 countries. Mortality was 36.9 percent in institutions that had longstanding ECLS programs in place prior to the pandemic and 58.9 percent in institutions that had not. Although formal data on the number of patients treated with ECLS in Canada are not available, it is estimated to be between 300 and 400 patients.
In addition to pneumonia, COVID-19 may cause pulmonary embolism (blood clots to the lungs), acute myocardial infarction, and strokes in some patients, who are treated with anticoagulants that inhibit the blood clotting. The virus that causes COVID-19 may also infect nervous tissues and has been shown to cause several neurological conditions including isolated neuropathies, such as Guillain Barre Syndrome and Acute Demyelinating Encephalomyelitis.
Patients with severe symptoms may have an overactive inflammatory system due to high circulating levels of pro-inflammatory cytokines; this may cause damage to the heart, blood vessels, and kidneys. Patients with this condition, known as multiple organ dysfunction syndrome (MODS) often require treatment for low blood pressure using vasopressors and inotropes, medications to maintain an adequate blood pressure.
Acute kidney injury (AKI) has been reported in 20 to 78 percent of critically ill patients with COVID-19 (Nadim et al. 2020) and 20 percent of COVID-19 patients in ICU required dialysis (Gupta et al. 2020).
Other treatments for hospitalized patients with COVID-19
In addition to supportive care for lung and other organ dysfunction, clinical trials involving patients with COVID-19 have investigated the effect of several direct antiviral medications, anti-inflammatory treatments, anticoagulants, and antibody-based treatments. The rapid scaling up of clinical trials has been both one of the greatest challenges and research success of the pandemic response.
Patients hospitalized because of COVID-19 requiring supplemental oxygen are typically treated with repurposed medications shown to reduce organ dysfunction and mortality, including anti-inflammatory corticosteroids, dexamethasone and the antiviral remdesivir.
Patients with severe COVID-19 and evidence of significant systemic inflammation may also receive other anti-inflammatory medications such as tocilizumab or sarilumab based on availability. Supplies of tociluzimab have been limited, however. In addition, patients hospitalized on medical wards, but not admitted to ICUs, appear to have reduced organ dysfunction and mortality when treated with systemic anticoagulation. (Science Table 2021. COVID-19 Advisory for Ontario 2021). Available at: covid19-sciencetable.ca/sciencebrief/#infectious-diseases-clinical-care. Accessed 11 October 2021).
Monoclonal antibodies, have been shown to reduce organ dysfunction and mortality, particularly when used early in high-risk patients and have been used with the hopes of reducing pressure on hospitals and ICUs (Lee 2021). However, these agents seem less effective against the omicron than earlier variants. The oral antiviral medication, Paxlovid, which is particularly effective in preventing severe disease in patients with COVID-19 infection, is a promising step towards developing more effective and easier to administer antiviral treatments for this disease. However, Paxlovid interacts adversely with medications for conditions including cardiovascular diseases, seizures, gout, and erectile dysfunction, which limits its use. Although Paxlovid is now widely available in Canada, its use has been surprisingly limited, likely due to the requirement to initially confirm the diagnosis with a molecular test at a time when these are increasingly difficult to access in many provinces. (Weeks 2022)
The dissemination of data from studies that have not undergone full peer review and publication has been both advantageous and problematic. The rapid distribution of the finding that dexamethasone improved outcomes in patients with hypoxemia caused by COVID-19 pneumonia was beneficial. However, the dissemination of data from poorly executed studies has led to increased misinformation on the value of medications such as hydroxychloroquine and ivermectin.
The absence of family visitation and presence at the bedside is associated with an increased incidence of delirium in ICU patients (Kandori et al. 2020; Pun et al. 2021; see section below). Because of this and many other reasons outlined in the section on the psychological impact of lack of visitation on ICU patients, family members and other support persons should be allowed to visit patients in the ICU.
What has been the impact on pediatric ICUs?
Background
As of 3 June 2022, 714,687 COVID-19 positive cases out of 3.74 million in Canada were in people 19 years of age or younger. Of these, 6,291 were hospitalized, 625 were admitted to ICU, and 50 died (Government of Canada 2022a, 2022b). However, the low incidence of ICU admission and mortality do not convey the impact that the COVID-19 pandemic has had on pediatric intensive care unit (PICU) resources. During the pandemic, PICU resources have been significantly impacted due to increased admission due to multi-inflammatory syndrome in children (MISC), child abuse and suicide attempts. Furthermore, the situation was exacerbated due to the redeployment of PICU staff to adult ICUs and long-term care facilities, delays in transportation of critically ill children to tertiary centres and delays or cancellations of surgeries requiring PICU beds.
There are only 16 PICUs with approximately 240 beds in Canada (Stiff et al. 2011) as they are only found in tertiary care, academic pediatric centres, whereas critically ill adult patients may be admitted to community hospitals (Fowler et al. 2015). Thus, for a population of 7.25 million children (≤ 18 years), there are 3.3 beds/100,000 children, lower than the 5.0-8.8 beds/100,000 children in several other G7 nations (Warncke et al. 2018; Horak et al. 2019).
There are no data on the ratio of appropriately skilled individuals needed to look after critically ill children although, the proportion of intensive care staff with the skills to intubate and insert vascular catheters in small children is undoubtedly considerably lower than those who care for critically ill adults. For example, the Royal College of Physicians and Surgeons of Canada General Internal Medicine competencies (Royal College of Physicians and Surgeons of Canada 2019) require general internal medicine residents to be able to insert peripheral arterial lines and obtain central venous access whereas the competencies for general pediatrics do not (Royal College of Physicians and Surgeons of Canada 2019). In addition, adult ICU nurses are less experienced at inserting intravenous catheters and obtaining blood samples from small children and infants and thus cannot easily replace PICU nurses during times of crisis.
PICU experience during the COVID-19 pandemic
In the first wave of the pandemic, between January and July 2020, 26 (3.2 percent) of the 811 patients admitted with COVID-19 were younger than 18 years, and 5 were admitted to PICU (Murthy et al. 2020); none of the pediatric patients died. However, the low incidence of vaccinations in the 12-17 age group and the inability to vaccinate younger children (American Academy of Pediatrics 2021), has led to an increase in the total number of PICU admissions for COVID-19 (Government of Canada 2021). There has been an increased rate of pediatric hospitalization and PICU admission following the arrival of the omicron variant, possibly due to its significantly increased transmissibility rather than an increased severity of illness. (Ulloa et al. 2022; Government of Canada 2022a, 2022b). A North American study found 40 percent of children admitted to PICU had medically complex conditions, almost one-quarter were immunosuppressed or had a malignant neoplasm, and 15 percent were obese. (Shekerdemian et al. 2020).
It is important to note that while the Government of Canada groups data for people 19 years old or less, most PICUs only accept patients less than 18 years of age (16 years of age or less in British Columbia, Manitoba). Consequently, there is a slight discrepancy between the data from the Government of Canada and this report.
Multi-inflammatory syndrome in children
The multisystem inflammatory syndrome in children (MISC), believed to be a hyper-inflammatory response to a preceding SARS-CoV2 infection (Henderson et al. 2022) became increasingly commonly reported two to six weeks after the first wave of the pandemic. Clinical presentations of patients with MISC vary from mild to requiring ECLS. A recent systematic review and meta-analysis found that 57.4 percent of patients diagnosed with this syndrome were admitted to hospital (8705/9335), 14.6 percent to PICU (1359/9335), and almost 1 percent died (96/9335) (Irfan et al. 2021). A recent study in 31 US states from March 15 to 31 October 2020, found that 398 patients with MISC and 253 with COVID-19 were admitted to participating PICUs, of which 18 patients required ECLS and 10 patients (1.9 percent) died (Feldstein et al. 2021). These data clearly highlight the importance of MISC in PICU resource utilization. A report from Public Health Ontario, based on 14 systematic reviews and 18 primary articles, found that 70-80 percent of patients with MISC required PICU care and 25 to 30 percent required mechanical ventilation. As of 1 August 2021, 15 of 16 Canadian PICUs reported having admitted 120 patients with suspected MISC. Data on the outcome of these patients are currently unavailable.
Extra-corporeal life support for COVID-19 related disease in children
Although the requirement for ECLS in children with COVID-19 infections or MISC is rare, it is important to note that 7 of the 16 academic pediatric centres in Canada are not able to provide this life-saving service. Furthermore, 3 of these PICUs (Janeway Children’s Health and Rehabilitation Centre in St. John’s, The Children’s Hospital of Winnipeg, and Jim Pattison Children’s Hospital in Saskatoon) are more than an hour away by plane from the nearest ECLS centre. Data for use of ECLS for COVID-19 and MISC in children are limited. A recent meta-analysis of adults noted that decreased age was associated with improved outcomes (Ramanathan et al. 2021), highlighting the importance of having this therapy available for younger patients.
Family presence in PICU during COVID-19 pandemic
While family presence is important for all critically ill patients, all 16 Canadian PICUs enacted site-specific policies to restrict family presence for variable time periods during the pandemic, even though this is crucial for children admitted to the PICU. Family members not only provide emotional support but as the primary caregivers, they provide much needed medical support and information for the care team (Baird et al. 2016; Sabeti et al. 2021). Furthermore, for split families with dual custody, consent for treatment is required from both parents with resulting treatment implications following the implementation of one visitor per patient policies. Researchers at the Izaak Walton Killam Hospital in Halifax are studying the impact of restricted family presence on PICU patients and their families during the pandemic and will develop evidence-based guidelines for consistent implementation of family presence in PICUs in the event of future threats. Mitigation strategies for future pandemics may include an increase in the number of isolation rooms (Mahoney et al. 2020) and use of telemedicine platforms (Ozawa et al. 2021); although the latter should not be viewed as a substitute to actual parental presence in the PICU (Sabeti et al. 2021).
Indirect consequences of COVID-19 on PICU admissions
During a year of lockdowns and school closures due to the COVID-19 pandemic, rising rates of child abuse and suicide attempts among Canada’s youth have sparked concern. McMaster Children’s Hospital reported a three hundred percent increase in admissions following a suicide attempt over a four-month period in 2021 compared to 2020. (Aziz 2021). However, Ray and colleagues (2022) found that the rates of self-harm, overdose, or death in adolescents was lower during than before the pandemic.
All 16 PICUs reported postponing or cancelling surgeries due to the pandemic, and The Hospital for Sick Children in Toronto reported a 24 percent increase in backlogs compared to the same time last year. Furthermore, recommendations such as, “Adequate time should be allowed for operating room cleaning and air filtration between surgical cases”, (Matava et al. 2020) resulted in fewer non-urgent surgical cases (e.g., elective cardiac surgery being performed) when post-operative recovery required admission in the PICU. In addition, dozens of hospitals in Ontario closed their pediatric wards and diverted children to tertiary care pediatric hospitals, increasing the ward burden for these hospitals and limiting transfer capabilities for patients out of the PICU (DeClerq 2021). The long-term impact of COVID-19, neurodevelopmental, psychosocial, and mental health outcomes on children are unknown, and are under study.
Adult patients in PICUs
Published recommendations suggest that critically ill adults should only be admitted to PICUs during a crisis surge response after the strategies for conventional and contingency responses have been exhausted (Einav et al. 2014). These include, but are not limited to, maximally expanding critical care capacity within hospitals by recruiting pediatric critical care staff and expertise to adult units, setting up temporary hospital structures and repurposing areas such as post-anesthetic recovery rooms.
Careful assessment of critical illness considering age and type of comorbidities has been suggested as a safe and effective approach for determining which COVID-19 patients are most appropriate for PICU admission (Gist et al. 2021). During the pandemic, PICUs in Canada admitted 80 adult COVID-19 patients aged 40 to 60 years of age with varying degrees of comorbidities, and 44 adult non-COVID-19 patients. It is important to note that this occurred on a background of a total of 240 PICU beds and during a time that several PICUs had deployed nurses to adult ICUs.
We have obtained limited information from individual PICUs on admissions of adult patients. The first adult was admitted in the Children’s Hospital of Eastern Ontario, Ottawa, PICU on 20 April 2021, and between then and 20 June 2021, when the last adult patient was discharged there were a total of 58 adult patient days of care. Health Sciences Children’s Hospital in Winnipeg admitted the first adult patient to the PICU on 8 April 2021, and the last adult patient was discharged on 18 June 2021. At Children’s Hospital of Saskatoon, the first adult patient was admitted to the PICU on 19 June 2021, and the last adult patient was discharged from the PICU on 23 February 2022. The PICU at the Stollery Children’s Hospital admitted adult patients from 20 December 2020, to 30 June 2021, and again from September 2021, with adult patients continuing to April 2022. No adult patients were admitted to the PICU at the Alberta Children’s Hospital, but staff were deployed to adult ICUs.
Significant time and resources were needed to prepare pediatric units to care for adult patients (Remy et al. 2020) as it not only required changes in medical equipment and drug dosing but had implications for resources required to support the delivery of critical care, including radiology, pharmacy, and laboratory services. Further considerations relating to care of larger and heavier adult patients included the need for larger beds, as well as the availability of patient lifts and increased staffing to manually lift and turn patients for prone positioning. In addition, the pediatric clinicians needed to be supported in-person or remotely by adult intensivists to provide input daily on rounds, as well as for complex decisions such as emergencies, resource reallocation, or end-of-life decisions (Einav et al. 2014).
The limited information available on the outcomes of adults with COVID-19 treated in adapted PICUs suggests that clinical outcomes were similar to those treated in adult ICUs (Sinha et al. 2021).
Redeployment of PICU staff
At least 7 of the 16 PICUs redeployed PICU nurses to adult ICUs and 2 of the 16 PICUs to long-term care (LTC) facilities. Several PICU staff deployed to LTC facilities contracted COVID-19 and were therefore unavailable to return for a protracted period, thus decreasing already limited staff for PICU patients.
Transport challenges
Four of 16 PICUs felt that the availability of transport for critically ill pediatric patients was insufficient during the pandemic. This was particularly evident in Ontario where critical care transportation was required to move upwards of 80 critically ill adult COVID-19 patients per day from the greater Toronto area to other parts of the province. This resulted in some pediatric patients remaining in isolated, under-resourced communities for much longer than was desirable.
The impact of the COVID-19 pandemic on PICU resources has likely been underestimated due to the focus on the relatively low number of cases of severe COVID-19 in children. The full impact of COVID-19 on PICUs in Canada has been further limited by lack of coordinated, national, real-time data collection in PICUs.
Recommendations:
(1) Although the PICUs provided substantial assistance to the care and outcomes of adults (Sinha et al. 2021), it may be more efficient to maximize adult ICU capacity and to send staff to the adult ICUs rather than send adult patients to PICUs.
(2) Strategies need to be implemented now to ensure appropriate use of adult and PICU resources during future crises.
What measures were employed by hospitals and health authorities to create extra ICU capacity?
Adaptations to provide critical care services during pandemic
Faced with an increased demand for ward and ICU beds, as well as for personnel to staff them during the COVID-19 pandemic, hospitals were forced to take several steps to avoid being overwhelmed when expanding ICU capacity. Many utilized existing disaster and emergency response planning resources (Christian et al. 2006; Christian et al. 2014) to guide the development of their surge plan to ensure sufficient space, supply, and staff to appropriately meet the needs of the incoming critically ill patients. It was possible to progressively increase the number of ICU beds in a hospital during a surge by using other spaces within the hospital and redeploying large numbers of non-ICU trained staff to these extra beds. However, as the number of ICU beds and dependence on non-ICU staff increases, inevitably the quality of care is put at risk and other hospital services are adversely impacted as their staff are redeployed (Cullen 2021). The care adaptations by hospitals and provincial health systems allowed staff, equipment, and space to be available to provide ICU care to the thousands of extra critically ill patients with COVID-19. However, these measures diverted those resources from many other patients.
A report estimates that over 500,000 surgical procedures were postponed across Canada from March 2021 to June 2021 (CIHI 2021a, 2021b), and that the number of surgeries decreased by approximately 35,000 a month during the first 16 months, with the largest declines during the first wave of the pandemic in early 2020.
Space
It was evident from the onset of the pandemic that an increase in critical care beds was required, and several strategies were rapidly implemented to achieve this. These included reducing demand for acute and critical care services by postponing scheduled procedures and surgeries requiring hospital ward or ICU resources (Al Mutair et al. 2020; Halpern and Tan 2020), discharging less acutely ill patients to the wards (Griffin et al. 2020) or to other facilities (Christian et al. 2006; Abir et al. 2020; Maves et al. 2020; Williams et al. 2020; Winkelman et al. 2021), and using telehealth to avoid transfers into overwhelmed COVID-19 centers (Abir et al. 2020; Bourgeault et al. 2020; Halpern and Tan 2020; Singh et al. 2021).
Many strategies were focused on converting single ICU rooms into double rooms, transforming acute care, peri-procedural care areas and simulation centers to acute COVID wards and ICU beds, caring of adult ICU patients in pediatric ICUs, and establishing mobile temporary hospital facilities (Abir et al. 2020; Cammerota et al. 2020; Carenzo et al. 2020; Griffin et al. 2020; Oakley et al. 2020; Schneider et al. 2020; Uppal et al. 2020; Arabi et al. 2021). In some instances, these newly designated ICU spaces required the installation of proper infrastructure and equipment such as high efficiency particulate (HEPA) filters, temporary structures to provide separate spaces for donning and doffing, medical gas outlets, and sufficient electrical power for critical care equipment. This retrofitting was costly and time-consuming, therefore using areas that already had these features, such as Post Anesthetic Care Units, High Dependency Units and Operating Rooms, was prioritized. However, in many instances, non-ICU clinical areas were converted without much retrofitting. Patients admitted for non-COVID-related illnesses were placed in rooms and open wards where they contracted the infection. Hospitals across Canada have reported significant numbers of such outbreaks that resulted in staff illness and deaths in vulnerable patients (Mitchell et al. 2021; Wong 2021; Vescera 2021; CTV News 2022).
While some hospitals have been overwhelmed, others in different regions had more capacity, resulting in some patients being transported greater than usual from their typical health care catchment area in order to have access to acute and critical care resources. For example, some patients in Ontario, British Columbia, Alberta, Saskatchewan, Québec, and Manitoba were transported to larger centers within the province. During severe surges, critically ill patients were transferred interprovincially in May/June 2021 from Manitoba to Ontario, Saskatchewan, or Alberta and in October 2021 from Saskatchewan to Ontario.
Equipment and supplies
The shortage of equipment and supplies was a major concern in the first wave of the pandemic. Many provinces struggled to secure sufficient stock of personal protective equipment (PPE), pharmaceuticals, ventilators, intravenous infusion pumps, and disposable materials. The need for provincial reserves and an efficient supply chain was apparent early on; most provinces established a control center where requests from health organizations would be submitted, processed, and supplies delivered based on need (Arabi et al. 2021).
New equipment was purchased when available, but other measures were required, such as reusing PPE, particularly N95 masks and visors (Abir et al. 2020; Schneider and Schneider 2020; Winkermann et al. 2021), or borrowing ventilators from other hospitals not yet affected by COVID-19. In addition, equipment such as anesthesia gas machines, transport ventilators, and ventilators used for non-invasive ventilation were repatriated from non-ICU settings to meet the increasing ICU demand, (Abir et al. 2020; Arabi et al. 2021; Aziz et al. 2020; Griffin et al. 2020; Uppal et al. 2020). To reduce or delay the need for intubation and ventilators, the use of high-flow nasal oxygen and non-invasive ventilation was encouraged when appropriate (Arabi et al. 2021). Similarly, a conservative approach to prescribing pharmaceuticals that were low in stock was often necessary, in addition to using alternative drug classes when feasible (Arabi et al. 2021).
The challenges that provinces and territories experienced in securing sufficient supplies throughout this pandemic highlighted the importance of maintaining up-to-date inventory in hospitals, reviewing supply chains and provincial stocks, and projecting potential gaps and needs in the event of a surge (Aziz et al. 2020; World Health Organization 2020; Arabi et al. 2021).
As hospitals focused on expanding critical care capacity by reallocating space and maximizing supplies and equipment, we quickly realized the limiting factor was the health workforce. Thus, focusing on the number of critical care beds and ventilators available without considering the trained and skilled professionals is unwise. We must consider the interconnectedness between bed capacity, supplies, equipment, and the healthcare workforce when surge planning (Halpern and Tan 2020).
Staff
Worldwide, critical care staffing shortages existed prior to the COVID-19 pandemic but have been greatly exacerbated since (Rose et al. 2007; Wynne et al. 2021). In preparation for the large influx of critically ill patients, the critical care workforce needed to augment its capacity while maintaining safe working conditions.
A variety of strategies were implemented across the country to meet the additional demands in critical care settings and COVID-19 units. From the onset, it was widely recognized that respecting the recommended nurse to respiratory therapist ratios may not be feasible in a crisis of this magnitude. One of the most widely used strategies was off-loading tasks to non-critical care trained staff to maintain patient safety (Al Mutair et al. 2020; Aziz et al. 2020; Halpern and Tan 2020). This was possible by suspending or decreasing many services, provided an opportunity to move staff to areas where the number of patients was increasing, such as in critical care, emergency departments, and COVID-19 medical units.
The goal for redeployed staff was not to achieve the knowledge or competency of a trained critical care nurse but to augment the ability of trained critical care nurses to deliver care to a larger number of critically ill patients (Al Mutair et al. 2020; Lauck et al. 2021). Many organizations deployed nurses with previous experience in critical care, or in areas that provided monitored care to assist critical care nursing staff. Models of care for redeployed staff included dyads, where a critical care nurse was paired with a non-critical care nurse, allowing them to provide care to two to three patients depending on the patients’ acuity (Lauck et al. 2021). Other forms of care-team models, or tiered staffing strategies, were used to provide care to a greater number of patients and reinforce ICU staff (Al Mutair et al. 2020; Arabi et al. 2021; Aziz et al. 2020; Halpern and Tan 2020). The principles guiding the model of care included patient safety and maximization of each nurse’s scope of practice and competencies (Lauck et al. 2021).
Training programs were established, and varied in length depending on health regions, individual units, as well as the learning needs of non-critical care staff. Many focused on PPE use, cardiac and arterial monitoring, mechanical ventilation, suctioning, and proning. Redeploying non-critical care to work with critical care staff increased the workforce but both parties recommended more formal processes for communication, planning, skillset inventory, and sharing of expectations (Lauck et al. 2021).
Other commonly used strategies included hiring retired, inactive or past employees with critical care training (Al Mutair et al. 2020; Griffin et al. 2020; Williams et al. 2020), providing on-the-spot or online training and simulations sessions for non-ICU clinicians reassigned to critical care (Aziz et al. 2020), and recruiting medical, nursing, and other health profession students who are nearing the end of their programs to provide caregiver support (Al Mutair et al. 2020; Williams et al. 2020). In hard-hit areas, Canadian Armed Forces’ support, intraprovincial and interprovincial assistance was requested, notably in Ontario, Alberta, and Manitoba (D’Mello 2021; McKendrick 2021; Rieger 2021; Williams et al. 2020; Global News, Govt of Canada 2021; Rieger 2020) to alleviate some of the burden. In April 2021, critical care nurses from Newfoundland came to Ontario (CBC News 2021), whereas in October 2021, critical care nurses from the Canadian Forces and the Canadian Red Cross were sent to Alberta during the severe surge of patients in that province (Konguavi and Frew 2021). To facilitate interprovincial mobility of critical care staff, licensing bodies either expedited the licensing process for incoming help or eliminated regulatory barriers altogether. For example, under the premise of the Emergency Management and Civil Protection Act, 1990, out-of-provinces nurses could practice in Ontario hospitals to support the fight against COVID-19 without the College of Nurses of Ontario licensing (Coghlan 2021).
To increase both critical care capacity and efficiency, many institutions opted to redistribute critical care-related tasks among other qualified clinicians. Examples include anesthesiologists inserting vascular access devices and artificial airways to alleviate the work of intensivists, and physicians or trainees with ventilator management experience supporting the work of respiratory therapists (Al Mutair et al. 2020; Griffin et al. 2020; Oakley et al. 2020; Arabi et al. 2021). Restructuring ICU teams through the implementation of a tiered staffing model was also used to increase the efficiency in the care provided and to safely care for the most patients possible (Al Mutair et al. 2020; Aziz et al. 2020). Lastly, short-term solutions, such as cancelling vacation and leaves, increasing working hours, increasing the number of patients per staff, and forcing overtime were also employed in some jurisdictions. However, these strategies risk impairing the mental and physical health of critical care workers (Williams et al. 2020; Arabi et al. 2021).
It has long been recognized that demand for ICU resources could exceed supply in a major pandemic, as seen with the influenza A(H1N1) pandemic in 2008/09. Consequently, many jurisdictions around the world, including Canada, drafted ICU triage protocols but these were never activated. Ontario, Québec, Saskatchewan, and Alberta modified those triage protocols for implementation if ICU capacity is overwhelmed by surges of critically ill patients with COVID-19 (Alberta Health Services 2021; Critical Care Ontario 2021; Government of Quebec 2020; Kirkey 2021; Valiani et al. 2020).
At different times during the pandemic there was extensive media coverage regarding the need to implement triage protocols in Québec, Ontario, Alberta and Saskatchewan (Favaro et al. 2021). However, activating these triage protocols was avoided by deploying non-ICU staff overseen by ICU professionals to work in auxiliary ICUs in post-anesthetic recovery areas, operating rooms, and other makeshift ICUs, or by transferring ICU patients out of province. However, many Canadian intensivists indicated they had to make challenging decisions on who to admit to their ICUs during this pandemic at times of bed and staff shortages (Rinaldi 2021). Currently, provincial triage protocols are generally similar, but there are important differences.
The standard of care inevitably suffered when hospitals and ICUs were overwhelmed with patients or when patients had to be transferred to ICUs thousands of miles away from their homes. (Wittnebel 2021). Studies from Canada and the United Kingdom reported higher ICU mortality, prolonged lengths of stay and increased ICU costs during times of high-capacity strain (Chrusch 2009; Bagshaw et al. 2018; Trans et al. 2019; Wilcox et al. 2020). There is also evidence to suggest that under such stressful conditions there are changes in approaches to patient care, including an increase of “Do Not Resuscitate” orders. (Stelfox et al. 2012)
The responsibility for delivering health and other social services rest largely with Provincial and territorial governments, resulting in different models of care, training, and credentialing across the country. In areas hardest hit by the pandemic, this has caused national, provincial, and regional challenges when it comes to sharing human resources. Future pandemic and surge planning should incorporate efficient processes for communication, rapid credentialing, and training to upskill workers between regions and provinces. This would allow safe and effective workforce mobility across the country. Furthermore, pandemic redeployment plans should include discussions with unions to facilitate the movement of staff to areas of greatest need with appropriate compensation for doing so. Lastly, pandemic plans must include processes to accurately predict staffing requirements based on projections of pandemic spread, while factoring in the loss of staff to illness, quarantine, and burnout. Options for rapidly scaling up the critical care workforce, while maintaining patient safety and care quality must also be included, with careful consideration to avoid devaluing the knowledge, skill and expertise required to care for critically ill patients (Bourgeault et al. 2020; Wynne et al. 2021).
Canadian Armed Forces’ role in critical care services during the pandemic
Canadian Armed Forces (CAF) deployed critical care nursing officers and medical technicians to hospitals and long-term care facilities in several provinces, to support Northern and Indigenous communities, help PHAC with distribution of PPE and to aid in contact tracing in Ontario (Government of Canada 2019). In addition, the military used a CC-130 Hercules aircraft equipped with an Aeromedical Bio-containment Evacuation System (ABES) to transport COVID-19 patients from Manitoba to Ontario (Global News 2021).
Operation LASER was the official CAF response to the pandemic (Government of Canada 2021) but did not specifically outline a plan for critical care support services. The military has the potential to augment civilian critical care services during future pandemics in three domains: personnel, field hospitals and transport.
The CAF Health Service has roughly 5,102 personnel which include clinical specialists, physicians, physician assistants, dentists, nurses, pharmacists, physiotherapists, health care administrators, and various technicians. Of these, approximately 400 nurses and 25 physicians have some critical care specialist training and could be deployed to ICUs in the country in times of crisis.
The Aeromedical Bio-containment Evacuation System (ABES) is a specially designed large isolation unit that fits in CC-130 Hercules and CC-177 Globemaster aircraft. This unit provides space where multiple infected patients can be kept and treated by medical staff, while ensuring the safety of the aircraft’s crew (Government of Canada 2020). This could be used to simultaneously transfer multiple patients more efficiently in a future crisis.
Recommendations:
1.
In addition to increasing ICU capacity and staffing as recommended above, a selected group of non-ICU nurses in each hospital should be trained in critical care and be available in the event of a major surge in patients requiring ICU care. Their skills should be maintained by intermittent scheduled shifts in the ICU.
2.
Provincial licensing bodies should be prepared to rapidly provide licenses for intensivists and other ICU health professionals from other provinces and territories in the event of a surge in demand for ICU beds.
3.
Health Canada, the Department of National Defence and provincial departments of health should prepare contingency plans for the evacuation of critically ill patients to ICUs in other provinces in the event a province’s ICUs are being overwhelmed.
4.
ICU Triage Plans should be standardized across all provinces and territories and the public should be made aware of their existence.
What is the impact of an ICU admission on survivors?
Post-Intensive Care Syndrome following COVID-19.
Post-intensive Care Syndrome (PICS) refers to physical, cognitive, and mental impairments that occur when both in the ICU and after discharge. A large proportion of seriously ill patients who survived but required prolonged mechanical ventilation and deep sedation than may impacted by PICS. This may impact the long-term quality of life of patients (Herridge et al. 2011; Hopkins et al. 2005; Rousseau et al. 2021) and often continue for prolonged periods of time (Graselli et al. 2020; Mitra et al. 2020; Yang et al. 2020).
The ICU patients at the highest risk of developing PICS often have a history of comorbidities such as diabetes, hypertension, obesity, chronic obstructive pulmonary disease, and (or) prolonged mechanical ventilation. A profile that is similar to that of COVID-19 patients with increased risk of developing critical illness. (Rodriguez-Morales et al. 2020). A recent study of ICU COVID-19 survivors found 87 percent had physical impairment, 48 percent had psychiatric impairments ranging from mild depression to post-traumatic stress disorder (PTSD), while 8 percent had impairments on cognitive screening (Martillo et al. 2019).
Six months after hospitalization with COVID-19, of 1,077 patients in the UK,71 percent described themselves as not having fully recovered, 20 developed a new disability, and 19 percent had a health-related change in occupation (Evans et al. 2021). Patients described a median of nine different physical and mental symptoms, which were similar in both patient-reported outcome measures and in objective physical assessments. Many of the patients who received care outside of ICU had symptoms identical to those seen in patients with PICS following ICU admission. This is not surprising as many seriously ill patients who would normally have been admitted to an ICU for therapies such as high flow oxygen have been cared for entirely in non-ICU, medical COVID-19 units. (Evans et al. 2021).
PICS also significantly affects the patient’s family members, decision-makers and long-term caregivers, classified as PICS-F (see below), many of whom suffer from post-traumatic stress disorder, anxiety, depression, and a diminished quality of life (Petrinec and Martin 2018).
The management, treatment, and education of patients and their families are essential in mitigating the long-term effects of critical care. The treatment of PICS begins in the ICU with sedation minimization and early mobilization followed by physical rehabilitation and psychiatric and psychological support that will likely be required for months. This will also require the necessary dedicated nursing, physiotherapy, and occupational therapy resources. (Teixeira Rosa 2018; Mayer et al. 2020).
As there are currently over 22,000 survivors of an ICU admission for COVID-19 in Canada, there will be an increasing need for the necessary outpatient supports being allocated to address the long-term impact on survivors (Public Health Agency of Canada 2022).
Recommendation
Increased funding should be allocated for the development and operation of specialized ICU Survivor Clinics to provide ongoing care in a holistic manner, including mental health issues, for patients with PICS.
What is the psychological impact on critical care professionals of working under such prolonged and severe pressures for 20 months?
Psychological impact of COVID-19 on health care professionals in ICUs
We are facing a new pandemic-related crisis in our hospitals, especially in our ICUs. While the pandemic has had a devastating effect on the patients and families of those who became critically ill and those who died, the effect on the healthcare professionals who cared for them twenty-four hours a day, seven days a week for 20 months has been profound. Some contracted the disease at work, many have suffered from long-COVID and from severe psychological injuries. Since the start of the pandemic, over 150,000 health care workers in Canada have developed COVID-19 and at least 46 health care workers have died from COVID-19 (as of 15 June 2021) (Canadian Institute for Health Information 2022a, 2022b).
Critical care professionals always face high levels of daily stress, heavy workloads, and constant readjustments to their work environment, all of which have been exacerbated during the COVID-19 pandemic. (Greenberg et al. 2021). The pandemic presented ICU, and indeed most health care system hospital staff across Canada, with a unique set of stressors for a prolonged duration.
On July 30th, 2021, a nurse posted on social media: “As an ICU nurse who loved this speciality, having COVID patients in the ICU was a war zone. One ICU room would now carry two patients. Short-staffed, our workload doubled, as we were also faced with a lack of personal protective equipment. Put your N95 mask in a paper bag and wear it every day with every patient for one full week. Gown and glove and face shields. As I interviewed several frontline ICU nurses in the aftermath of COVID, I watched them talk to me with their heads hanging low and with monotone voices, and I heard the same replies. Anxiety. Depression. Defeat. Death.” (Moore-Black and Kevin 2021)
Initially, stressors were related to a lack of specific resources such as shortages of PPE, availability of ICU beds, ventilators, medications, and limited staffed ICU bed capacity, whereas in the later stages the stressors have been related to human resources (nurses, doctors, and allied professionals). This led to earlier than recommended discharge of patients to avoid spread of infection, and to create capacity for new patients. This resulted in insufficient time to provide optimal care to all patients and increasing psychological harm to caregivers. Health care workers were concerned that exposure could result in a requirement for quarantine or cause illness, which caused further anxiety as they were aware that any absenteeism will further burden colleagues.
Each day ICU staff are exposed to traumatic situations that place them at risk of burnout, compassion fatigue, moral distress, and suffering, as well as PTSD. (For the definitions of the above please refer to Appendix A). The pandemic has exacerbated these risks and has led to a greater incidence of depression, anxiety, thoughts of self-harm, or alcohol abuse (Greenberg et al. 2021).
Thirty five percent of health care workers looking after COVID-19 patients have self-reported insomnia and low sleep quality. Preti and colleagues reported that 45 percent of health care workers presented with severe anxiety symptoms affecting psychological well-being associated with increasing levels of distress, decreasing sleep quality and self-efficacy (Preti et al. 2020). In a recent study assessing mental health of nurses in a Canadian ICU during the COVID-19 pandemic, the participants reported clinical concern for (23 percent), probable (13 percent) and significant (38 percent) symptoms of post-traumatic stress disorder, as well as mild to severe depression (57 percent), anxiety (67 percent) and stress (54 percent). (Crowe et al. 2021).
Studies following the 2003 SARS outbreak provided insight into the range of mental health and stress-related issues likely to impact critical care staff during a pandemic (Preti et al. 2020). Up to 3 years after the SARS pandemic, about 14 percent of interviewed hospital staff showed moderate depressive symptoms while 8.8 percent reported high symptoms (Liu et al. 2012). Lancee et al. (2008) reported that 5 percent of Toronto health care workers in Toronto had psychiatric disorders 1 to 2 years after the end of the SARS pandemic.
A similar study in China showed that 15.4 percent of respondents showed significant mental health symptoms one year after the end of the SARS pandemic (Lung et al. 2009). There are several reports indicating infection-related concerns from health care workers with regards for personal and family health during the SARS, MERS, and H1N1 pandemics (Goulia 2010; Alsubaie et al. 2019; Nickell et al. 2004).
Risk factors for psychological injury
Studies have shown that physicians were less worried about infection compared to other health care workers. Nurses reported higher perceived stress levels (Hines et al. 2021; Lief et al. 2018) and psychopathological symptoms (Matsuishi et al. 2012) including PTSD symptoms (Lai et al. 2020; Maunder et al. 2004). At least in part, this different may be due to the higher physical contact that nurses have with patients.
Given the nature of the interventions and constant interaction with patients in ICU, it is considered a high-risk infection work environment (Costa and Moss 2018). Thus, it is not surprising that during SARS and MERS health care workers in units where there was a high risk of infection presented more severe mental health outcomes than those in low-risk units (Matsuishi et al. 2012; McAlonan et al. 2007). During the COVID-19 pandemic non-ICU trained nurses redeployed to the ICU appeared to be a specific mental health risk factor. Conversely, voluntarily accepting the risk of infection may be a protective factor (Preti et al. 2020). Crowe et al. (2021) identified rapidly changing policy and information, overwhelming and unclear communication, meeting patients’ care needs in new ways while staying safe, managing home and personal commitments to self, and family as factors leading to psychological distress.
The death of ICU COVID-19 patients may be further traumatic events for critical care staff, especially nurses, as they spend long hours with patients, often under enduring unusual and “cold” circumstances (lack of presence of family, inability to hold patient’s hands without PPE, etc.). It has been reported that a patient’s emotional and physical distress and perceived quality of death also psychologically impact on nurses. Additionally, unrealistic family expectations may be another source of distress (Wong et al. 2005).
Additional stressors for ICU healthcare professionals have been dealing with unvaccinated patients or those denying the existence of COVID-19, sometimes aggressive families demanding unproven therapies, and protestors outside obstructing entry to the hospitals.
Protective factors
Measures that have been proposed to combat mental health issues related to stress, include organizational support and adequate training (Lancee et al. 2008), confidence in the effectiveness of personal protective equipment and infection control measures (Chua et al. 2004) and burnout (Maunder et al. 2006). In addition, a supportive framework for decision-making and individual priorities, while upholding ethical considerations, is crucial in reducing the severity of moral distress in ICU staff (Plouffe et al. 2021).
Particular attention should be given to nurses, since results show that they are especially affected by their prolonged exposure to infected patients (Preti et al. 2020). Resilience factors such as having a strong sense of purpose, ability to adapt and cope, positive mental state, confidence, optimism, and strong social support will lead to a healthier workforce that will likely show better psychological responses in future emergency situations (Crowe et al. 2021).
Interventions
Faced with intense psychological pressure and strain, it is not uncommon to develop maladaptive strategies such as denial, isolation, compartmentalization, excessive eating, gambling, and substance abuse. To mitigate and reduce such risks, it is necessary to provide effective, easily accessible psychosocial support and interventions now and post-pandemic. Critical care staff should be provided with the tools and skills to build resilience, improve their adaptive coping capacity and emotional wellbeing. Resilience refers to one’s ability to adapt and “bounce back” after dealing with stress or challenging situations (Malik et al. 2021).
There are many excellent virtual platforms and mobile apps available to address self-care, wellness, and stress management. In addition, psychological treatments such as Cognitive Behavioral Therapy, Mindfulness-Based Stress Reduction, Acceptance and Commitment Therapy, and Eye Movement Desensitization and Reprocessing are all extremely effective in dealing with sleep disturbance, anxiety, depression, grief reactions and PTSD. (Hofmann et al. 2017; Sander et al. 2020; David et al. 2018; Kabat-Zinn 2003; Penque 2019). Regular peer support and structured group meetings should be encouraged to optimize coping during challenging and stressful times. If necessary, individual treatment with a psychologist or psychiatrist should be facilitated.
Another recommended method to identify the early warning signs of distress and quickly provide support is Psychological First Aid, which has been used for many years by the military and during critical incidents, to provide guidance as well as tools and strategies in a non-judgemental way. This resource is for individuals who are competent, but nevertheless are feeling overwhelmed (Lief et al. 2018; Blake 2020; Fessell et al. 2020).
Summary
The COVID-19 pandemic continues to have a psychological and physical impact on health care workers, especially the ICU staff dealing with the sickest patients. There is an epic level of burnout in healthcare workers resulting in significant staff shortages (Grant 2021; Tomblin-Murphy et al. 2022; Hollingsworth and Schulte 2021).
Recommendations
As the pandemic continues and afterwards, healthcare organizations need to examine ways in which they can adapt their health workplace practices to:
1.
Implement strategies to reduce moral and psychological distress by actively monitor the well-being of the critical care staff to ensure that the impacts of workload changes are properly understood and mitigated where possible.
2.
Prioritize staff mental health support and timely access to evidence-based treatments.
3.
Recognize the benefits of self-care and self-compassion for all interprofessional team members.
4.
Obtain additional funding from all government levels to support health care workers mental and physical health.
5.
Organizational wellness and health programs should be amended and adapted to offer critical care workers assistance coping with the consequences of working in a pandemic.
What is the psychological impact of restrictions on family visitation during a pandemic?
Prior to COVID-19, a “family centered” approach was the norm when dealing with the critically ill in ICU, optimizing support and open communication with family members. Rapport and trust were established with the ICU staff and this model of collaboration enhanced the ability to face and deal with difficult treatment options and end of life decisions. Family members were at the bedside with their loved ones at the time of death. The ability to hold their hand and provide comforting rituals helped with bereavement and the mourning process (Hart et al. 2021; Boulton et al. 2022). Having family at the bedside is a psychological protective factor for patients, family, and ICU staff (Mistraletti et al. 2021; Hugelius et al. 2021; Diolaiuti et al. 2021).
Katie Hafner (2020) wrote “Of all the ways the coronavirus pandemic has undermined the conventions of normal life, perhaps none is as cruel as the separation of seriously ill patients and their loved ones, mandated at hospitals around the world. While the infection control rationale is clear and sound, the consequences for patients, their loved ones and the hospital personnel who must enforce the rules are profound”.
Clinicians and hospital staff report that keeping patients’ families away had been among the darkest experiences of their professional lives. The restrictions run contrary to a hospital’s desire to keep patients and families together for the salutary effect of something as simple as handholding, or a chair pulled close to a bed. In addition, having a relative present can also ease the workload of a medical team, and in some cases they may provide crucial information that a confused patient cannot (Hafner 2020)
Awdish and Ely (2020) wrote “That excluding families and loved ones from the bedside of the sickest COVID patients, leads to immense trauma to families due to being excluded from essential moments of their loved one’s illness, recovery and dying process that would allow understanding and healing. The absence of families will have long consequences on care teams, they poignantly observe: So much of our joy in work comes from developing relationships with families and working together for the best outcomes. Families can motivate patients… and serve as advocates and they need to be present at bedside for their own mental wellbeing. Phone calls, even by facetime, are a feeble surrogate for what the family really needs”.
During the initial phases of the COVID-19 pandemic, when family hospital visits were restricted or outright banned, the only mode under these circumstances was “cold” communication, via telephone and video conferencing. This decreased the quality of the communication and clinicians felt that this was harmful for patients and family members (Azoulay et al. 2020; Kentish-Barnes et al. 2021)
Why is in-person interaction so important? Face-to-face communication has always been a crucial element of our lives (Hoehl et al. 2021) The sound of spoken words, observing body language, eye contact, and facial gestures give a better understanding and connection between the critical care staff and the family member. Family centered guidelines in times of crisis are warranted, the presence of family members in ICU’s should remain a priority (Davidson et al. 2017).
Post intensive care syndrome in families (PICS-F)
Stress reactions consistent with a high risk of developing PTSD is common in family members of adult and pediatric ICU patients (up to 33 percent) and family members of patients who died in the ICU are at a higher risk (up to 50 percent). Perceived inadequate information by ICU physicians (48 percent) and involvement in end-of-life decisions (60 percent), are independent determinants of the risk for post-traumatic stress reaction. (Azoulay et al. 2005).
Post Intensive Care Syndrome (PICS) may also be present in family members and is known as PICS-F. (Rawal et al. 2017) The major causes of PICS-F are poor communication, a role as critical decision maker, educational level, and facing life and death situations with their loved ones. A lack of interaction between caregivers and families induces a feeling of exclusion and significant emotional burden when patients die. (Robert et al. 2020). Family members reported frustration, anger, confusion, feelings of hopelessness, guilt, anxiety, and at times lack of trust in the critical care staff when visits were restricted. Virtual platforms were also problematic because of digital literacy, language barriers and socioeconomic inequities (Munshi et al. 2021; Jones-Bonofiglio et al. 2021).
For relatives, witnessing terminal dyspnea and not being able to say goodbye to a loved one can result in psychological sequelae, like PTSD-related symptoms in the former and complicated grief symptoms in the later (Kentish-Barnes et al. 2015; Robert et al. 2020) Prolonged grief disorder is a chronic mental health issue that requires treatment and should be differentiated from depression, grief, mourning and bereavement (American Psychiatric Association 2013).
During a pandemic there is a disruption in social norms, end of life rituals, and usual mourning practices (Mayland et al. 2020). In their recent study of family members of patients who died in an ICU during the COVID-19 pandemic, Kentish-Barnes et al. (2021) identified 3 major themes:
1.
Difficulty in building a relationship with the ICU clinicians and understanding the medical information.
2.
Distance communication was not sufficient, and participants reported increased feelings of solitude. A perceived deficit of communication was associated with a breakdown in the trust placed in the institution. Family members felt a lack of support and empathy when information was received over the phone.
3.
Family members experienced discontinuities and interruptions in the relationship with their loved one.
When banned from visiting, family members experienced feelings of powerlessness, abandonment, and unreality, rather than feeling they had an active role in the care of their loved ones. Participants felt it essential that patients did not die alone, and for some, visiting only at the end of life was perceived as insufficient.
Absence of these important rituals resulted in disruption of the normal grieving process, feelings of guilt, and what family members describe as “stolen moments” (Kentish-Barnes et al. 2021).
The ICU team
There is also the issue at the collective team level when ICUs were required to create new visiting protocols that included designating one or two family members as support caregivers, demonstrating the proper use of PPE, increased demand for communication and supplying information to families. These all led to increased demands/workload to an already overextended and tired critical care staff (Hugelius et al. 2021).
There was further psychological strain on critical care staff who became surrogates for family members. Jones-Bonofiglio et al. (2021) described the heartbreaking experiences of nurses, physicians, and anesthetists who were with patients at the end of life without family members present. These experiences can result in psychological injury, depression, moral distress, and post traumatic symptoms (Greenberg et al. 2021; Hart and Taylor 2021; Azoulay et al. 2005).
Tyler Dawson of the National Post, quoted Dr. Neeja Bakshi, an internist at the Royal Alexandra Hospital in Edmonton. “What bothers us - or torments us, I guess - is that these patients often are alone, and nobody should die alone, but it is also difficult that we have the volume that we have… You can’t be with every single person” (Dawson 2021).
In summary, it is difficult to reconcile the need for infection control practices, with the inherent limitations to family ICU visits, while at the same time the need of families desperately seeking information about their loved ones’ condition, and the idea of family centered care for these patients.
Recommendations
1.
Family members and close friends should be able to visit patients in the ICU.
2.
Mental Health Liaison Teams should be developed to facilitate and assist families navigating the system, and to ensure they receive appropriate mental health support in the community. The team could include social workers, clergy, volunteers, and retired medical and mental health professionals. This service may be especially relevant in assisting those patients and families experiencing psychosocial, psychological, and cognitive sequelae associated with PICS and PICS-F.
Canada’s critical care research agenda related to COVID-19
Thanks to the efforts of the Canadian Institute of Health Research (CIHR) to facilitate and to mobilize Canada’s health research community, several Canadian-led international trials contributed important knowledge to our understanding of COVID-19. Important examples include the Antithrombotic Therapy to Ameliorate Complications of COVID-19 trial, led by the Universities of Manitoba and Toronto, which showed the benefit of therapeutic anticoagulation among ward patients with COVID-19 and the finding of harm among those in the intensive care unit; the Together Trial, which is evaluating outpatient therapies and has been led by a leadership team in Canada but is recruiting patients in Brazil, the Canadian Treatments for COVID-19 trial in collaboration with the World Health Organization Solidarity Trial and the Randomized, Embedded, Multifactorial Adaptive Platform trial (REMAP) of which Canada is an international partner. (Lawler et al. 2021; REMAP-CAP investigators 2021; Reisick et al. 2021). Canadian centres also recruited patients to several international trials (Skipper et al. 2020; Pan et al. 2021). There are limited examples of large Canadian-led studies that took place primarily in Canada CONCOR-1 and COLCOT trials (Tardif et al. 2021; CONCOR-1).
However, the pandemic has also made it evident that there are major foundational deficiencies in health research in Canada. Lamontagne and colleagues stated that the root cause of the currently inadequate Canadian research infrastructure is the commonly held view that health research and health care are separate entities that should exist in their own silos. (Lamontagne et al. 2021). They believe a discussion on consequence of not having clinical research within Canadian health systems is needed and advocated for its integration into our health systems. They concluded that better healthcare depends on evidence informed decision-making and, therefore, on high-quality clinical research responsive to the systems’ needs. In their opinion, Canada’s limited research success during the pandemic has highlighted a broken system.
Tsang and colleagues commented that the COVID-19 pandemic has uncovered long-standing deficiencies in Canada’s clinical research infrastructure. For example, while many Canadian hospitals are participating in COVID-19-related research, most patients are cared for in centres that were not involved in clinical trials. (Tsang et al. 2021). As a result, recruitment to pandemic trials in Canada has been slow relative to other developed countries and the proportion of patients enrolled in clinical trials has been relatively low.
Chornecki and colleagues recently surveyed existing hospital, regional, provincial, and national data platforms to identify gaps and barriers in data collection. They found that the CIHI Health Information Discharge Abstract Database contains high-level clinical data on every adult and child discharged from acute care facilities but nothing on critical care-specific severity of illness risk-adjustment scores, physiologic data, or data pertaining to medication use. They also noted a very limited national infrastructure to collect and link biological samples from critically ill patients. They concluded that clinical and biological data collection among critically ill patients in Canada is not sufficiently coordinated, and lags other jurisdictions. (Chornecki et al. 2020).
Schwartz and colleagues noted that Canada’s research contributions during the pandemic were limited for several other reasons, most related to complex requirements and slow bureaucratic components. These included the time to obtain research ethics board approvals at many sites, funding, and the completion of contracts, even when expedited. These delays resulted in missed research opportunities at the start of the pandemic or meant that study questions had already been answered by investigators elsewhere. In addition, project-based funding calls have often been uncoordinated, and have tended to encourage individual investigators to individually embark on studies to answer similar questions rather than work collaboratively or be asked to join networks or respond to targeted research priority areas. Another significant limiting factor affecting the successful completion of research studies was the redeployment of researchers back to the bedside when hospitals and health systems were under severe stress due to patient surges. (Schwartz et al. 2021; McMahon et al. 2020).
Misleading clinical evidence, preprints of studies prior to peer review and false meta-analyses showing benefit of therapies such as ivermectin and colchicine have hampered the performance of properly performed randomized clinical trials and encouraged off-label use of these medications (Garegnani et al. 2021).
During the pandemic, Health Canada has been helpful and efficient in getting trials vetted and approved but having a fully national, collaborative, and binding research ethics approval process, like the United Kingdom, Australia, and New Zealand, would have significantly decreased the time needed for trial start up. A standard trial contract agreement template, pre-vetted by the sponsoring institution and research institutes would, perhaps, be the greatest regulatory opportunity to improve the time-to-initiation of trials.
Recommendations
1.
Clinical research must be integrated into and across our health systems.
2.
A discussion should be initiated on the lack of clinical research within Canadian health systems and its consequences.
3.
That clinical and biological data for research purposes should be collected nationally.
4.
A standard trial contract agreement template should be available at research institutes across Canada.
What have we learned?
The COVID-19 pandemic has challenged our ability to deliver life-saving acute and critical care to Canadians more than any other illness in our recent history. It has exposed the precarious demand-capacity balance in Canadian health care where, even under non-pandemic conditions, capacity just matches demand during most periods of the year.
CIHI (2019) found that ICUs in teaching hospitals and large urban hospitals had an average occupancy of 90 percent and 86 percent, respectively, indicating that for significant periods, such as during “influenza season” in the winter and during a busy “trauma season” in the spring and summer, occupancy was at 100 percent. High ICU occupancy, particularly above 80 percent, were associated with an increase in ICU mortality, hospital mortality, and ICU readmission within seven days of discharge. Therefore, an average occupancy of no higher than 80 percent has been recommended, to be able to respond to surges in demand (Chrusch et al. 2009; Capuzzo et al. 2014; Tierney and Conroy 2014).
During past outbreaks for SARS-COV-1 in 2003, and Influenza A(H1N1) in 2009-2010, it was evident that small increases in demand could overwhelm the acute health care system (Fowler et al. 2003; Smetanin et al. 2009). The COVID-19 pandemic has demonstrated that a prolonged increase in demand on acute and critical care overwhelms Canada’s ability to provide acute healthcare. This, in turn, drives the public health responses, leading to limitation in travel, population lockdowns, the closing of many businesses, and a significant negative impact on the economic and social structure of the country. ICU capacity, particularly human resources, has emerged as a critical bottleneck not only with respect to providing care for patients in need, but also to support continued social and economic activities in the population overall.
Even business systems that function economically and efficiently, using a lean systems approach with “just in time” production and delivery of goods, have been impacted significantly by supply chain disruptions during the pandemic. It is evident that our health systems, and definitely ICUs, cannot function with this model and need to have built in flexibility and resilience. From both a health system and broader economic perspective, this is a key learning from the pandemic in many countries around the world.
In addition to needing to augment public health and acute health care capacity in Canada, this pandemic has shown the need and value of cooperation, for without the regional and inter-provincial/territorial cooperation and transportation of critically ill patients, many more patients would have suffered or died from an inability to receive the care they needed. This underlines the necessity for our federally supported but provincially/territorially administered system of acute care to be more nationally connected, and perhaps federally incentivized as a component of the transfer payment system.
The availability of effective vaccines against COVID-19 dramatically changed the nature of the pandemic. During the fourth wave, caused by the delta variant, heavy demands were placed on the overall acute care system, and particularly on ICUs. This was most evident in western Canada where in some remote rural areas and select urban neighbourhoods there was a low incidence of vaccination, and high levels of COVID-19 infections. COVID-19 vaccines are over 90 percent effective against the delta variant and its precursors, but only 70 percent effective against severe infection by omicron (Collie et al. 2022). The omicron variant caused astonishingly high levels of community infection and the highest incidence of hospitalization but, as in other countries, Canadian ICU admissions were significantly lower in Canada than in previous waves of the pandemic. Sheikh et al. (2022) reported that while the incidence of serious breakthrough infections requiring ICU admission in Scotland was somewhat higher with omicron, the existing mRNA vaccines still exerted a significant protective effect particularly following a booster dose and have been effective in reducing the burden of serious illness requiring hospitalization, ICU admissions, and death. However, unvaccinated people are currently almost six times more likely to be hospitalized and almost 12 times more likely to require care in the ICU than a person who has received two or three doses (Ontario Science Table 2022). To state it simply, the best way to prevent our ICUs from being overwhelmed at some time in the future, is to maintain a high level of immunization, including booster shots, in the population. However, the arrival of the omicron variant with multiple spike protein mutations has underlined the possibility of mutations that not only increase transmissibility but could also be associated with more severe disease. This is most likely to happen in areas of the world that have low incidences of vaccination and high levels of infection.
Readiness to conduct the research required to establish effective national treatment for any new illness is essential for an effective health system response. The most efficient mechanism to achieve this is to establish a durably funded national acute and critical care network. This would consist of investigators and research coordinators, well integrated into our national clinical health systems, who conduct clinical trials, with pre-existing research ethics and contract agreements. National funders, regulators, research ethics boards, and researchers must be ready to respond immediately to a declared public health crisis with input from patients, the population, and other stakeholders. In addition, involved stakeholders need to establish focused national observational and experimental research priorities that will allow the network to focus on appropriate research protocols that will definitively answer questions, rather than having many individual and uncoordinated projects.
We know that pandemics have long-lasting effects on patients, health care workers and the general population. An important element of this pandemic response should now be focused on preventing and treating post-COVID-19 syndrome in patients, supporting the mental and physical health of health care workers, and solidifying the national research infrastructure needed to respond to the next health care crisis.
How should we move forward?
We must not forget what we have learned and be prepared for the next highly pathogenic variant and the next pandemic.
The National Advisory Committee on SARS and Public Health (Government of Canada 2004) noted we had much to learn from the outbreak of SARS, in large part because too many earlier lessons had been ignored.
In 2006, Mr. Justice Archie Campbell, Chair of the SARS Commission wrote:
“SARS taught us lessons that can help us redeem our failures. If we do not learn the lessons to be taken from SARS, however, and if we do not make present governments fix the problems that remain, we will pay a terrible price in the face of future outbreaks of virulent disease” (Campbell A 2007; The SARS Commission 2007).
Canada needs to understand the impact of the COVID-19 pandemic on the country and to prepare for the next pandemic. This pandemic has caused the deaths of 41,354 Canadians over 26 months, compared with 45,500 dying over more than five and half years during World War II. Viruses are jumping across species constantly and this is likely to occur more frequently as humans encroach on other species’ habitats. Future pandemics will inevitably happen and will likely be caused by novel pathogens that may be more deadly than COVID-19.
High levels of immunity to COVID-19 must be maintained in the Canadian population.
It is important to encourage all adult Canadians to become fully immunized against COVID-19, as defined by having 3 doses of vaccine (two for those under 18 years). This will reduce the impact on ICUs during any future waves as the vaccines are highly protective against the development of serious illness resulting in a need for ICU admission.
Canada’s ICU capacity must be expanded significantly.
Singapore, Portugal, and Spain, have a higher incidence of immunization than Canada, but continue to struggle with ongoing surges of COVID-19, so we will probably see a similar trend although, hopefully, at a lower level of severity (CNA 2021; Demony and Vicente 2021; Johns Hopkins University 2021). Consequently, each province must consider how to increase the number of staffed ICU beds to provide invasive mechanical ventilation and multiple organ support. In the first instance, this will require accurate regular reporting of the number of staffed, funded ICU beds available for critically ill mechanically ventilated patients. Subsequently, funding will be required to expand existing ICUs and build new ones, as well for the increased numbers of healthcare professionals required. This will require careful consideration at all levels of government and federal financial support. The eventual model would see an average occupancy in Canadian ICUs of no more than 80 percent, but with the ability to rapidly increase to 200 percent of regular occupancy in the event of a severe surge or another pandemic. Since most ICUs in Canada have operated at or close to 100 percent occupancy prior to the pandemic, this would require at least a 20 percent increase in ICU beds nationally, but some provinces will require a significantly higher increase as their current ICU capacity is so low.
Critical care professionals must be valued, retained and new professionals recruited.
New hospitals and ICUs are of little value without trained health professionals to work in them. Even prior to the pandemic, there was a shortage of nurses. Global nursing leaders, nursing associations and nursing unions have been warning of an impending workforce shortage, especially in ICUs, during the remainder of this pandemic and into the future (Alharbi et al. 2020; Credland 2021; Kurth et al. 2021). Canada faces the same risks to its critical care nursing and RT workforce (Grant 2021; Miller et al. 2021). Because of the stress, many ICU staff are struggling, many have left their positions, and some are leaving the profession entirely. A recent report indicated that two thirds of nurses working at the Royal Inland Hospital in Kamloops, British Columbia had left their positions (Letterio 2021) and likely more will leave in the coming months. Miller et al. showed that 35 percent of respondents were seriously considering leaving the profession due to inadequate staffing, inability to complete work, high workloads, and poor leadership. This escalation of burnout, the decrease in undergraduate enrollment, and the increase in retirements are leading to a decline in Canadian RT numbers.
A recent, yet unpublished survey of critical care nurses identified the following potential strategies to improve retention and recruit new staff:
•
Additional mental health resources to cope with the added psychological burden from the pandemic which is in addition to the normal day-to-day mental health burden. These resources include mentoring and peer support groups, PTSD prevention and coping strategies, psychological support focusing on coping, and building resilience as supports that would be of benefit for all critical care staff.
•
Improving working environments by better staffing ratios, decreasing workplace violence, discontinuing mandatory overtime, and providing more management support at the frontline.
•
Educational programs that focus on the clinical knowledge required to work in an ICU, and the tools needed to develop resiliency should be available to ICU nurses.
•
Hospitals and provincial health authorities should partner with Canadian Universities to include ICU clinical rotations in their curriculum to entice new nursing graduates to a rewarding career in critical care as a specialty.
The pandemic has also highlighted specific problems inherent in a female-dominated profession such as nursing. These include accessible childcare, which was identified as a barrier by many of the survey respondents. With the lockdowns during the pandemic, daycare access became limited and affected nurses’ ability to be available for work. This highlights a need for employers to focus on flexible work schedules and improved childcare options for shift workers.
The impact of the ongoing pandemic on the critical care workforce cannot be minimized. It is imperative that governments, hospitals, and health authorities implement strategies to retain and recruit this immensely valuable highly skilled workforce to ensure the delivery of quality care to Canadians that require care in our ICUs (Silas and Smith 2021).
Canadian hospitals must be upgraded.
Many older hospitals in Canada struggled during waves of the pandemic to even provide an adequate and consistent flow of oxygen under the burden of the numbers of seriously and critically ill patients. In November 2020, Alberta Health Services advised hospitals in Calgary to reduce oxygen use in anticipation of further COVID-19 patients being admitted (Rieger 2021), while patients at Michael Garron Hospital in Toronto were transferred to other hospitals because of concerns that oxygen supplies would be exhausted due to the number of COVID-19 patients being treated (McGillivary et al. 2021). The HVAC systems in many older hospitals do not meet the current standard of 12 air exchanges per hour. The design of new hospitals must prevent airborne transmission of pathogens as some patients admitted with other illnesses were placed in rooms and open wards and contracted COVID-19 (Greenhalgh et al. 2021; Centers for Disease Control and Prevention 2021). Furthermore, many ICUs had to place two patients in cubicles built and equipped to care for one patient (Keller 2020). It is time to seriously evaluate the state of our acute care hospitals in Canada and determine how we can upgrade our infrastructure to modern standards where necessary and to construct modern, state-of-the-art hospitals.
New hospital buildings must be acuity adaptable.
As new hospitals and wings are planned and constructed across Canada, careful consideration should be given to incorporating acuity adaptability into their design and functionality. This will require that regular medical/surgical units have additional gas, vacuum, power, and data outlets so that they can be easily converted to ICUs. In addition, there should be hidden gas, vacuum, power plumbing, and data outlets in non-clinical areas, such as conference rooms, underground car parks, and even entrance hallways, to enable those areas to become medical units in the event of a pandemic (France 2021; Simone 2020; Rush University 2021; Simone 2021).
We must understand that SARS-CoV-2 is not finished with us.
It was widely hoped the pandemic would be nearing an end as a result of immunization and natural infection, but it is now clear this virus and its descendants are not yet finished with us. Very recent data (see Appendix) show we are entering a sixth wave of COVID-19 hospitalizations even before patients hospitalized during the fifth wave have left the hospitals. The appearance of the omicron variant and its many subvariants shows that the virus has the capacity to mutate frequently and to create variants that can evade the immunity provided by our vaccines. Although the omicron variant and its subvariants have caused fewer infected individuals to become seriously ill, it is so much more transmissible that hospital systems have been put under severe pressure. It has been widely stated that as viruses evolve, they tend to become more efficient at transmission but cause less serious illness. However, in reality, RNA viruses such as SARS-CoV-2 mutate in a random fashion so while the most successful variants are more easily transmitted, there is no reason they cannot also cause more serious disease. In fact, a higher incidence of transmission increases the probability of new mutations, potentially resulting in even more virulent strains.
In a best-case scenario, COVID-19 will eventually become endemic, that is, the infection is regular, present intermittently on a seasonal basis, and predictable. However, COVID-19 becomes endemic, it is critical that diagnostic testing capacity is not lost, that appropriate stores of personal protective equipment are maintained, and that health systems remain capable of responding to new surges of the disease.
The federal and provincial governments must conduct honest and open in-depth reviews of their pandemic responses and initiate the development of a system of coordinated responses.
Provinces varied greatly with regards to when and how they implemented public health restrictions and vaccination mandates. Despite pleas from intensivists and public health experts, some provinces delayed implementation of effective public health measures. This resulted in needless deaths and the eventual requirement to evacuate critically ill patients to ICUs in other provinces. Some provinces prematurely discontinued public health measures and ignored pleas from experts as COVID-19 cases surged. These actions serve as a precautionary tale on how not to manage a pandemic. It is evident that it is unwise to rely on vaccines alone, particularly when the incidence of vaccination is low and when the threat of new vaccine-resistant variants is real. It is also apparent that the timing of initiation and removal of public health measures is vital to manage the severity of surges of severe illness due to COVID-19.
Formal mechanisms to ensure consistency in public health responses, critical care capacity and ICU triage protocols across Canada including rapid licensing requirements for health professionals redeployed between provinces, must be put in place. The Government of Canada must be prepared to enact the necessary emergency powers to protect the citizens of Canada regardless of where they live.
Competing interests
The authors have declared that no competing interests exist.
References
Abir M, Nelson M, Chan EW, Al-Ibrahim H, Cutter C, Patel KV, et al. 2020. Critical Care Surge Response Strategies for the 2020 COVID-19 Outbreak in the United States. RAND Corporation, Santa Monica, CA. [online]: Available from rand.org/pubs/research_reports/RRA164-1.html.
Aiken LH, Sloane DM, Bruyneel L, Heede KVD, Griffiths P, Busse R, et al. 2014. Nurse staffing and education and hospital mortality in nine European countries: a retrospective observational study. Lancet. 383(9931): 1824–1830.
Al Mutair A, Amr A, Ambani Z, Salman KA, Schwebius D. 2020. Nursing Surge Capacity Strategies for Management of Critically Ill Adults with COVID-19. Nurs Rep. 10(1): 23–32.
Alberta Health Services: Critical Care Triage Protocol. 2021. [online]: Available from albertahealthservices.ca/scns/Page13849.aspx
Alharbi J, Jackson D, Usher K. 2020. The potential for COVID-19 to contribute to compassion fatigue in critical care nurses. J Clin Nurs. 29(15–16): 2762–2764.
Alsubaie S, Hani Temsah M, Al-Eyadhy AA, Gossady I, Hasan GM, Al-rabiaah A, et al. 2019. Middle East Respiratory Syndrome Coronavirus epidemic impact on healthcare workers’ risk perceptions, work and personal lives. J Infect Dev Ctries. 13(10): 920–926.
American Academy of Pediatrics Children and COVID-19: State-Level Data Report. 2022. [online]: Available from aap.org/en/pages/2019-novel-coronavirus-covid-19-infections/children-and-covid-19-state-level-data-report/
American Psychiatric Association. 2013. Diagnostic and statistical manual of mental disorders (5th ed.).
Arabi YM, Azoulay E, Al-Dorzi HM, Phua J, Salluh J, Binnie A, et al. 2021. How the COVID-19 pandemic will change the future of critical care. Intensive Care Med. 47(3): 282–291.
Awdish R and Ely EW. 2020. Keeping loved ones from visiting our coronavirus patients is making them sicker. [online]: Available from washingtonpost.com/outlook/2020/08/06/coronavirus-icu-patients-families/
Aziz S, Arabi YM, Alhazzani W, Evans L, Citerio G, Fischkoff K, et al. 2020. Managing ICU surge during the COVID-19 crisis: rapid guidelines. Intensive Care Med. 46(7): 1303–1325.
Aziz S. 2021. Child abuse, suicide attempts in Canada rose during COVID-19 pandemic: report. [online]: Available from globalnews.ca/news/8157443/covid-children-abuse-suicide-canada-report/
Azoulay E, Cariou A, Bruneel F, Demoule A, Kouatchet A, Reuter D, et al. 2020. Symptoms of Anxiety, Depression, and Peritraumatic Dissociation in Critical Care Clinicians Managing Patients with COVID-19. A Cross-Sectional Study. American Journal of Respiratory and Critical Care Medicine 202(10): 1388–1398.
Azoulay E, Pochard F, Kentish-Barnes N, Chevret S, Aboab J, Adrie C, et al. 2005. FAMIREA Study Group. Risk of post-traumatic stress symptoms in family members of intensive care unit patients. American Journal of Respiratory and Critical Care Medicine 171(9): 987–994.
Bagshaw SM, Wang X, Zygun DA, Zuege D, Dodek P, Garland A, et al. 2018. Association between strained capacity and mortality among patients admitted to intensive care: A path-analysis modeling strategy. J Crit Care. 43: 81–87.
Baheti AD, Nayak P. 2022. Covid-19 in India: Oxygen shortages and a real-world trolley problem. The BMJ 376: o369.
Baird J, Rehm RS, Hinds PS, Baggott C, Davies B. 2016. Do You Know My Child? Continuity of Nursing Care in the Pediatric Intensive Care Unit. Nurs Res. 65(2): 142–150.
Barbaro RP, MacLaren G, Boonstra PS, Combes A, Agerstrand C, and Annich G, et al. 2021. Extracorporeal membrane oxygenation for COVID-19: evolving outcomes from the international Extracorporeal Life Support Organization Registry. Lancet, 398(10307): 1230–1238.
Barrett KA, VandeVyvere C, Haque N, Gao M, Yan S, Lebovic G, et al. 2021. Critical care capacity during the COVID-19 pandemic. Science Briefs of the Ontario COVID-19 Science Advisory Table, 2(51).
Bennett D. 2022. Alberta to spend $300M on new critical care beds. [online]: Available from cbc.ca/news/canada/calgary/alta-critical-care-beds-1.6370437
Blake N. 2020. Caring for the Caregivers During the COVID-19 Pandemic. AACN Adv Crit Care. 31(4): 416–418.
Bloomer MJ, Fulbrook P, Goldsworthy S, Livesay SL, Mitchell, ML, Williams G, et al. 2019. World Federation of Critical Care Nurses 2019 Position Statement: Provision of a Critical Care Nursing Workforce. Connect: The World of Critical Care Nursing, 13: 3–7.
Booth A, Reed AB, Ponzo S, Yassaee A, Aral M, Plans D, et al. 2021. Population risk factors for severe disease and mortality in COVID-19: A global systematic review and meta-analysis. PLoS One 16(3): e0247461.
Boulton AJ, Jordan H, Adams CE, Polgarova P, Morris AC, Arora N. 2022. Intensive care unit visiting and family communication during the COVID-19 pandemic: A UK survey. Journal of the Intensive Care Society.
Bourgeault IL, Maier CB, Dieleman M, Ball J, MacKenzie A, Nancarrow S, et al. 2020. The COVID-19 pandemic presents an opportunity to develop more sustainable health workforces. Human Resources for Health, 18(1): 83.
Cambell A. 2007. Spring of Fear. The SARS Commission Report. [online]: Available from archives.gov.on.ca/en/e_records/sars/report/v1.html.
Cammarota G, Ragazzoni L, Capuzzi F, Pulvirenti S, Vita ND, Santangelo E, et al. 2020. Critical Care Surge Capacity to Respond to the COVID-19 Pandemic in Italy: A Rapid and Affordable Solution in the Novara Hospital. Prehosp Disaster Med. 35(4): 431–433.
Canadian Association of Critical Care Nurses. 2017. Standards for Critical Care Nursing Practice (5th ed.) [online]: Available from caccn.ca/publications/standards-for-critical-care-nursing-practice/
Canadian Association of Critical Care Nurses. 2019. Position Statement: Models of Nursing Care in Critical Care. [online]: Available from caccn.ca/publications/practice-guidelines-position-statements/
Canadian Institute for Health Information. 2020. Hospital Beds Staffed and In Operation, 2018–2019. CIHI, Ottawa, ON. [online]: Available from docs.google.com/viewer?url=https%3A%2F%2Fwww.cihi.ca%2Fsites%2Fdefault%2Ffiles%2Fdocument%2Fbeds-staffed-and-in-operation-2018-2019-en-web.xlsx
Canadian Institute for Health Information. 2021a. Nursing in Canada, 2020 — Data Tables. [online]: Available from cihi.ca/sites/default/files/document/nursing-in-canada-2011-2020-data-tables-en.xlsx.
Canadian Institute for Health Information. 2021b. Comparing estimated costs of COVID-19 hospitalizations and other common hospitalizations in Canada, January 2019 to March 2020, and January 2020 to March 2021. [online]: Available from cihi.ca/en/covid-19-and-other-common-conditions-comparing-hospital-costs
Canadian Institute for Health Information. 2022a. COVID-19’s impact on hospital services [online]: Available from cihi.ca/en/covid-19-resources/impact-of-covid-19-on-canadas-health-care-systems/hospital-services.
Canadian Institute for Health Information. 2022b. COVID-19 Cases and deaths in health care workers in Canada. [online]: Available from cihi.ca/en/covid-19-cases-and-deaths-in-health-care-workers-in-canada.
Canadian Medical Association. 2019. Critical care medicine profile. [online]: Available from cma.ca/sites/default/files/2020-10/critical-care-e.pdf
Canadian Nurses Association. 2019. RN workforce profile by area of responsibility – year 2019. [online]: Available from cna-aiic.ca/en/nursing/regulated-nursing-in-canada/nursing-statistics
Canadian Society of Respiratory. 2021. Therapists. The rt profession. [online]: Available from csrt.com/wp-content/uploads/What-is-an-RT_2019.pdf)
Capuzzo M, Volta C, Tassinati T, Moreno RP, Valentin A, Guidet B, et al. 2014. Hospital mortality of adults admitted to intensive care units in hospitals with and without Intermediate Care Units: a multicentre European cohort study. Critical Care 18(5): 551.
Carenzo L, Costantini E, Greco M, Barra FL, Rendiniello V, Mainetti M, et al. 2020. Hospital surge capacity in a tertiary emergency referral centre during the COVID-19 outbreak in Italy [published correction appears in Anaesthesia. Anaesthesia, 75(7): 928–934.
CBC News. 2021. Team of N.L. ‘health-care heroes’ heading to Ontario on Tuesday. CBC news [online]: Available from cbc.ca/news/canada/newfoundland-labrador/nl-health-care-ontario-help-1.6001999
Centers for Disease Control and Prevention. 2021. Scientific Brief: SARS-CoV-2 Transmission. [online]: Available from cdc.gov/coronavirus/2019-ncov/science/science-briefs/sars-cov-2-transmission.html.
Chamberlain D, Pollock W, and Fulbrook P. 2018. ACCCN Workforce Standards Development Group. ACCCN Workforce Standards for Intensive Care Nursing: Systematic and evidence review, development, and appraisal. Aust Crit Care. 31(5): 292–302.
Channel News Asia. 2021. Singapore reports 3,474 new COVID-19 cases and 7 more deaths. [online]: Available from channelnewsasia.com/singapore/covid-19-moh-nov-17-new-cases-deaths-2319631.
Chornenki JN, Liaw P, Bagshaw S, Burns K, Dodek P, English S, et al. 2020. Data initiatives supporting critical care research and quality improvement in Canada: an environmental scan and narrative review. Bases de données étayant la recherche et l’amélioration de la qualité des soins intensifs au Canada: une étude générale de la situation et revue narrative. Can J Anaesth. 67(4): 475–484.
Christian MD, Devereaux AV, Dichter JR, Rubinson L, Kissoon NTask Force for Mass Critical Care, et al. 2014. Task Force for Mass Critical Care. Introduction and executive summary: care of the critically ill and injured during pandemics and disasters: CHEST consensus statement. Chest 146(4 Suppl): 8S–34S.
Christian MD, Wax R, Lazar N, Hawryluck L, Herridge M, Fortie W, et al. 2006. Critical Care During a Pandemic Final report of the Ontario Health Plan for an Influenza Pandemic (OHPIP). Ontario Minister of Health and Long-Term Care.
Chrusch CA, Olafson KP, McMillan PM, Roberts DE, and Gray PR. 2009. High occupancy increases the risk of early death or readmission after transfer from intensive care. Crit Care Med. 37(10): 2753–2758.
Chua SE, Cheung V, Cheung C, McAlonan GM, Wong JW, Cheung EP, et al. 2004. Psychological effects of the SARS outbreak in Hong Kong on high-risk health care workers. Canadian Journal of Psychiatry. Revue Canadienne de Psychiatrie 49(6): 391–393.
Clay RA. 2021. Are You Experiencing Compassion Fatigue? American Psychological Association (APA). 1–6. [online]: Available from apa.org/topics/covid-19/compassion-fatigue
Coelho P. 2020. Relationship Between Nurse Certification and Clinical Patient Outcomes: A Systematic Literature Review. J Nurs Care Qual. 35(1): E1–E5.
Coghlan, A. 2021. IMPORTANT UPDATE: New provincial orders – change to scope of practice in hospitals. College of Nurses of Ontario. [online]: Available from cno.org/en/news/2021/april-2021/important-update-new-provincial-orders--change-to-scope-of-practice-in-hospitals/
Collie S, Champion J, Moultrie H, Bekker LG, and Gray G. 2022. Effectiveness of BNT162b2 Vaccine against Omicron Variant in South Africa. New England Journal of Medicine 386(5): 494–496.
Conley P. 2019. Certified and Advanced Degree Critical Care Nurses Improve Patient Outcomes. Dimensions of Critical Care Nursing, 38(2): 108–112.
Costa DK, and Moss M. 2018. The cost of caring: emotion, burnout, and psychological distress in critical care clinicians. Annals of the American Thoracic Society, 15(7):787–790.
Credland, N. 2021. The sheer goodwill of staff only goes so far. Nursing Standard. 36(2): 13–13.
Critical Care Ontario. 2021. OC3PR: Maximizing care through an emergency standard of care. [online]: Available from criticalcareontario.ca/?s=triage.
Crowe S, Howard AF, Vanderspank-Wright B, Gillis P, McLeod F, Penner C, and Haljan G. 2021. The effect of COVID-19 pandemic on the mental health of Canadian critical care nurses providing patient care during the early phase pandemic: A mixed method study. Intensive and Critical Care Nursing, 63: 102999.
CTV news. 2021. Military to support Saskatchewan with up to six critical care nursing officers. [online]: Available from ctvnews.ca/health/coronavirus/military-to-support-saskatchewan-with-up-to-six-critical-care-nursing-officers-1.5636523.
Cullen P. 2021. What happens if ICU beds run out in Irish hospitals. Irish Times. [online]: Available from irishtimes.com/life-and-style/health-family/what-happens-if-icu-beds-run-out-in-irish-hospitals-1.4732519.
D’Mello C. 2021 April 16. Ontario turns to other provinces for ‘urgently needed’ help with overloaded ICUs. CTV news. [online]: Available from toronto.ctvnews.ca/ontario-turns-to-other-provinces-for-urgently-needed-help-with-overloaded-icus-1.5390044
David D, Cristea I, and Hofmann SG. 2018. Why cognitive behavioral therapy is the current gold standard of psychotherapy. Frontiers in Psychiatry 29(9): 4.
Davidson JE, Aslakson RA, Long AC, Puntillo KA, Kross EK, and Hart J, et al. 2017. Guidelines for family-centered care in the neonatal, pediatric, and adult icU. Critical Care Medicine, 45(1): 103–128.
Dawson T. 2021. Nobody should die alone’: Alberta doctor haunted by the faces of the COVID dead. National Post. [online]: Available from nationalpost.com/news/canada/dreaming-about-deaths-what-burnout-looks-like-for-albertas-doctors-battling-the-fourth-wave.
Dean W, Talbot S, and Dean A. 2019. Reframing clinician distress: moral injury not burnout. Federal Practitioner, 36(9): 400–402.
DeClerq K. 2021. Paediatric patients in GTA to be transferred to SickKids for care in effort to free space in hospitals. CTV News, [online]: Available from toronto.ctvnews.ca/paediatric-patients-in-gta-to-be-transferred-to-sickkids-for-care-in-effort-to-free-space-in-hospitals-1.5383855.
Demony C and Vicente P. 2021. Portuguese PM warns restrictions may return as COVID cases rise. [online]: Available from reuters.com/world/europe/portuguese-pm-warns-restrictions-may-return-covid-cases-rise-2021-11-16/
Detsky AS, and Bogoch II. 2021. COVID-19 in Canada: Experience and Response to Waves 2 and 3. JAMA, 326(12): 1145–1146.
Diolaiuti F, Marazziti D, Beatino MF, Mucci F, and Pozza A. 2021. Impact and consequences of COVID-19 pandemic on complicated grief and persistent complex bereavement disorder. Psychiatry Research, 300: 113916.
Einav S, Hick JL, Hanfling D, Erstad BL, Toner ES, Branson RD, et al. 2014. Surge capacity logistics: care of the critically ill and injured during pandemics and disasters: CHEST consensus statement. Chest, 146(4 Suppl):e17S–43S.
Elkrief A, Desilets A, Papneja N, Cvetkovic L, Groleau C, Lakehal YA. et al. 2020. High mortality among hospital-acquired COVID-19 infection in patients with cancer: A multicentre observational cohort study. European Journal of Cancer 139:181–187.
Epstein EG, Haizlip J, Liaschenko J, Zhao D, Bennett R, and Marshall MF. 2020. Moral Distress, Mattering, and Secondary Traumatic Stress in Provider Burnout: A Call for Moral Community. AACN Advanced Critical Care, 31(2): 146–157.
Evans RA, McAuley H, Harrison EM, Shikotra A, Singapuri A, Sereno M, et al. 2021. PHOSP-COVID Collaborative Group. Physical, cognitive, and mental health impacts of COVID-19 after hospitalisation (PHOSP-COVID): a UK multicentre, prospective cohort study. The Lancet Respiratory Medicine, 9(11): 1275–1287.
Faggioni MP, González-Melado FJ, and Di Pietro ML. 2021. National health system cuts and triage decisions during the COVID-19 pandemic in Italy and Spain: ethical implications. Journal of Medical Ethics,
Favaro, A, St. Philip, E, and Cousins, B. 2021. Ontario hospitals on the verge of enacting ‘last resort’ triage protocols. CTV News [online]: Available from ctvnews.ca/health/coronavirus/ontario-hospitals-on-the-verge-of-enacting-last-resort-triage-protocols-1.5406746
Feldstein LR, Tenforde MW, Friedman KG, Newhams M, Rose EB, Dapul H, et al. 2021. Characteristics and Outcomes of US Children and Adolescents With Multisystem Inflammatory Syndrome in Children (MIS-C) Compared With Severe Acute COVID-19. JAMA, 325(11): 1074–1087.
Fessell D, Cherniss Cand Coronavirus Disease. 2020. 2019 (COVID-19) and Beyond: Micropractices for Burnout Prevention and Emotional Wellness. J Am Coll Radiol. 17(6): 746–748.
Figley, CR. (Editors). 2002. Treating compassion fatigue. Brunner-Routledge.
Fitzsimmons MG, and Crowley J. 2022. COVID-19: Extracorporeal membrane oxygenation (ECMO). [online]: Available from uptodate.com/contents/covid-19-extracorporeal-membrane-oxygenation-ecmo/print.
Fowler RA, Abdelmalik P, Wood G, Foster D, Gibney N, Bandrauk N. et al. 2015. Critical care capacity in Canada: results of a national cross-sectional study. Critical Care 19(1): 133.
Fowler RA, Lapinsky SE, Hallett D, Detsky AS, Sibbald WJ, Slutsky AS, et al. 2003. Critically ill patients with severe acute respiratory syndrome. JAMA, 290(3): 367–373.
France. 2021. Israeli hospital transforms car park into virus ward. [online]: Available from france24.com/en/20200923-israeli-hospital-transforms-car-park-into-virus-ward.
Garegnani LI, Madrid E, and Meza N. 2021. Misleading clinical evidence and systematic reviews on ivermectin for COVID-19. BMJ Evidence-Based Medicine, 290(3): 367–373.
Gill FJ, Leslie GD, Grech C, and Latour JM. 2012. A review of critical care nursing staffing, education and practice standards. Australian Critical Care, 25(4): 224–237.
Gist RE, Pinto R, Kissoon N, Ahmed YE, Daniel P, Hamele M. 2021. Repurposing a PICU for Adult Care in a State Mandated COVID-19 Only Hospital: Outcome Comparison to the MICU Cohort to Determine Safety and Effectiveness. Frontiers in Pediatrics, 9: 665350.
Global news. 2021. Medically equipped Hercules plane to transport Manitoba ICU patients to other provinces [online]: Available from globalnews.ca/news/7901445/medically-equipped-hercules-plane-to-transport-manitoba-icu-patients-to-other-provinces/
Global news. 2021. Military begins work at Edmonton hospital as Alberta battles 4th COVID-19 wave [online]: Available from globalnews.ca/news/8246882/alberta-covid-19-military-edmonton/
Goulia P, Mantas C, Dimitroula D, Mantis D, Hyphantis T. 2010. General hospital staff worries, perceived sufficiency of information and associated psychological distress during the A/H1N1 influenza pandemic. BMC Infectious Diseases, 9(10): 322.
Government of Canada. 2004. The national advisory committee on sars and public health [online]: Available from canada.ca/en/public-health/services/reports-publications/learning-sars-renewal-public-health-canada/executive-summary.html#conclusion.
Government of Canada. 2016. 3214 – Respiratory therapists, clinical perfusionists and cardiopulmonary technologists. National Occupational Classification [online]: Available from noc.esdc.gc.ca/Structure/NocProfile?objectid=w4muX8TzyoHCYPBkCH307PEjKy3gjwnGg1%2BtG22Tn9s%3D
Government of Canada. 2019. Individual and community-based measures to mitigate the spread of COVID-19 in Canada. [online]: Available from canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/health-professionals/public-health-measures-mitigate-covid-19.html.
Government of Canada. 2020. Ensuring Safe Aeromedical Evacuations in the Global Era of Infectious Diseases [online]: Available from canada.ca/en/department-national-defence/maple-leaf/defence/2020/05/ensuring-safe-aeromedical-evacuations-in-the-global-era-of-infectious-diseases.html.
Government of Canada. 2021. COVID-19: Main modes of transmission. [online]: Available from canada.ca/en/public-health/services/diseases/2019-novel-coronavirus-infection/health-professionals/main-modes-transmission.html.
Government of Canada. 2021. Military response to COVID-19. [online]: Available from canada.ca/en/department-national-defence/campaigns/covid-19-military-response.html.
Government of Canada. 2021. Operation Laser. [online]: Available from canada.ca/en/department-national-defence/services/operations/military-operations/current-operations/laser.html.
Government of Canada. 2022a. Daily epidemiological summary [online]: Available from health-infobase.canada.ca/covid-19/epidemiological-summary-covid-19-cases.html.
Government of Canada. 2022b. Canada commits $2 billion in additional health care funding to clear backlogs and support hundreds of thousands of additional surgeries [online]: Available from canada.ca/en/department-finance/news/2022/03/canada-commits-2-billion-in-additional-health-care-funding-to-clear-surgery-and-diagnostics-backlogs.html.
Government of Quebec. 2020. Priorisation pour l’accès aux soins intensifs (adultes) en contexte extrême de pandémie (cmq.org).
Grant K. 2021. Canadian nurses are leaving in droves, worn down by 16 merciless months on the front lines of COVID-19. The Globe and Mail. [online]: Available from theglobeandmail.com/canada/article-canadian-nurses-are-leaving-in-droves-worn-down-by-16-merciless-months/
Grasselli G, Zangrillo A, Zanella A, Antonelli M, Cabrini L, Castelli A, et al. 2020. Baseline Characteristics and Outcomes of 1591 Patients Infected With SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA, 323(16): 1574–1581.
Greenberg N, Weston D, Hall C, Caulfield T, Williamson V, and Fong K. 2021. Mental health of staff working in intensive care during Covid-19. Occupational Medicine (Oxford, England) 71(2): 62–67.
Greenhalgh T, Jimenez JL, Prather KA, Tufekci Z, Fisman D, and Schooley R. 2021. Ten scientific reasons in support of airborne transmission of SARS-CoV-2. Lancet. 397(10285): 1603–1605.
Griffin KM, Karas MG, Ivascu NS, and Lief L. 2020. Hospital Preparedness for COVID-19: A Practical Guide from a Critical Care Perspective. American Journal of Respiratory and Critical Care Medicine, 201(11): 1337–1344.
Gupta S, Hayek SS, Wang W, Chan L, Mathews KS, and Melamed ML, et al. 2020. Factors Associated With Death in Critically Ill Patients With Coronavirus Disease 2019 in the US. JAMA Internal Medicine, 180(11): 1436–1447.
Hafner K. 2020. A heart wrenching thing: hospital bans on visits devastate families. [online]: Available from nytimes.com/2020/03/29/health/coronavirus-hospital-visit-ban.html
Halm M. 2021. Specialty Certification: a path to improving outcomes. American Journal of Critical Care, 30: 156–160.
Halpern NA, and Tan KS. 2020. United States resource availability for COVID-19. Society of Critical Care Medicine. [online]: Available from sccm.org/Blog/March-2020/United-States-Resource-Availabilityfor-COVID-19
Harbrecht BG, Delgado E, Tuttle RP, Cohen-Melamed MH, Saul MI, and Valenta CA. 2009. Improved outcomes with routine respiratory therapist evaluation of non-intensive-care-unit surgery patients. Respiratory Care, 54(7): 861–867.
Hardingham LB. 2004. Integrity and moral residue: nurses as participants in a moral community. Nurs Philos. 5(2): 127–134.
Hart JL, and Taylor SP. 2021. Family presence for critically ill patients during a pandemic. Chest, 160(2): 549–557.
Henderson LA, Canna SW, Friedman KG, Gorelik M, Lapidus SK, Bassiri H, et al. 2022. American College of Rheumatology Clinical Guidance for Multisystem Inflammatory Syndrome in Children Associated With SARS-CoV-2 and Hyperinflammation in Pediatric COVID-19: Version 3. Arthritis and Rheumatology, 74(4): e1–e20.
Herridge MS, Tansey CM, Matté A, Tomlinson G, Diaz-Granados N, Cooper A, et al. 2011. Functional disability 5 years after acute respiratory distress syndrome. New England Journal of Medicine, 364(14): 1293–304.
Hines SE, Chin KH, Glick DR, and Wickwire EM. 2021. Trends in Moral Injury, Distress, and Resilience Factors among Healthcare Workers at the Beginning of the COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 18(2): 488.
Hoehl S, Fairhurst M, and Schirmer A. 2021. Interactional synchrony: signals, mechanisms and benefits. Social Cognitive and Affective Neuroscience, 16(1–2): 5–18.
Hollingham R. 2022. How intensive care units were born. [online]: Available from bbc.com/future/article/20200610-how-intensive-care-units-were-born.
Hollingsworth H, and Schulte G. 2021. Health workers once saluted as heroes now get threats. AP News. [online]: Available from apnews.com/article/coronavirus-pandemic-business-health-missouri-omaha-b73e167eba4987cab9e58fdc92ce0b72.
Hofmann SG, and Gómez AF. 2017. Mindfulness-Based Interventions for Anxiety and Depression. Psychiatric Clinics of North America, 40(4): 739–749.
Hopkins RO, Weaver LK, Collingridge D, Parkinson RB, Chan KJ, Orme JF Jr. 2005 Two- year cognitive, emotional, and quality-of-life outcomes in acute respiratory distress syndrome. American Journal of Respiratory and Critical Care Medicine, 171(4): 340–347.
Horak RV, Griffin JF, Brown AM, Nett ST, Christie LM, Forbes, ML. 2019. et al. Growth and Changing Characteristics of Pediatric Intensive Care 2001-2016. Critical Care Medicine, 47(8): 1135–1142.
Howell BAM. 2021. Battling Burnout at the Frontlines of Health Care Amid COVID-19. AACN Advanced Critical Care 32(2): 195–203.
Hugelius K, Harada N, and Marutani M. 2021. Consequences of visiting restrictions during the COVID-19 pandemic: An integrative review. International Journal of Nursing Studies, 121:104000.
Institute of Medicine (US) Forum on Microbial Threats. 2007. Ethical and Legal Considerations in Mitigating Pandemic Disease: Workshop Summary. National Academies Press (US). 3, Strategies for Disease Containment, Washington (DC). [online]: Available from ncbi.nlm.nih.gov/books/NBK54163/
Irfan O, Muttalib F, Tang K, Jiang L, Lassi ZS, and Bhutta Z. 2021. Clinical characteristics, treatment and outcomes of paediatric COVID-19: A systematic review and meta-analysis. Archives of Disease in Childhood, 106(5): 440–448.
Johns Hopkins University Medicine Coronavirus Resource Center. 2021. [online]: Available from coronavirus.jhu.edu/vaccines/international.
Jones-Bonofiglio K, Nortjé N, Webster L, Garros D. 2021. A practical approach to hospital visitation during a pandemic: Responding with compassion to unjustified restrictions. American Journal of Critical Care, 30(4): 302–311.
Kabat-Zinn J. 2003. Mindfulness-based interventions in context: Past, present, and future. Clinical Psychology: Science and Practice, 10: 144–156.
Kandori K, Okada Y, Ishii W, Narumiya H, Maebayashi Y, and Iizuka R. 2020. Association between visitation restriction during the COVID-19 pandemic and delirium incidence among emergency admission patients: a single-center retrospective observational cohort study in Japan. Journal of Intensive Care Medicine, 8: 90.
Keller J. 2020. The Globe and Mail.
Kelly FE, Fong K, Hirsch N, and Nolan JP. 2014. Intensive care medicine is 60 years old: the history and future of the intensive care unit. Clinical Medicine journal (London). 14(4): 376–379.
Kendall-Gallagher D, and Blegen MA. 2009. Competence and certification of registered nurses and safety of patients in intensive care units. American Journal of Critical Care, 18(2): 106–114.
Kentish-Barnes N, Chaize M, Seegers V, Legriel S, Cariou A, and Jaber S. et al. 2015. Complicated grief after death of a relative in the intensive care unit. Eur Respir J. 45(5): 1341–1352.
Kentish-Barnes N, Cohen-Solal Z, Morin L, Souppart V, Pochard F, and Azoulay E. 2021. Lived Experiences of Family Members of Patients with Severe COVID-19 Who Died in Intensive Care Units in France. JAMA Network Open. 4(6): e2113355.
Kentish-Barnes N, Morin L, Cohen-Solal Z, Cariou A, Demoule A, and Azoulay E. 2021. The lived experience of icu clinicians during the coronavirus disease 2019 outbreak: A qualitative Study. Critical Care Medicine, 49(6): e585–e597.
Kirkey S. 2021. A plan of last resort: Choosing who lives and dies if ICUs turn into virus war zones. Montreal Gazette. [online]: Available from montrealgazette.com/news/canada/a-plan-of-last-resort-choosing-who-lives-and-dies-if-icus-turn-into-virus-war-zones
Kollef MH, Shapiro SD, Clinkscale D, Cracchiolo L, Clayton D, Wilner R, and Hossin L. 2000. The effect of respiratory therapist-initiated treatment protocols on patient outcomes and resource utilization. Chest, 117(2): 467–75.
Konguavi T and Frew N. 2021. Military nurses to land in Alberta Monday to ease health-care strain from COVID-19. CBC News. [online]: Available from cbc.ca/news/canada/edmonton/alberta-military-covid-19-hospital-icu-1.6197926
Kurth A, Pinker E, Martinello RA, Honan L, Choi S, and Beckman B. 2021. Critical care nursing: a key constraint to COVID-19 response and healthcare now and in the future. The Journal of Nursing Administration, 51(3): E6–E12.
Lai J, Ma S, Wang Y, Cai Z, Hu J, Wei N, et al. 2020. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Network Open, 3(3): e203976.
Lamontagne F, Rowan KM, and Guyatt G. 2021. Integrating research into clinical practice: challenges and solutions for Canada. CMAJ: Canadian Medical Association Journal 193(4): E127–E131.
Lancee WJ, Maunder RG, and Goldbloom DS. 2008. Coauthors for the Impact of SARS Study. Prevalence of psychiatric disorders among Toronto hospital workers one to two years after the SARS outbreak. Psychiatric Services, 59(1): 91–95.
Lauck SB, Bains VK, Nordby D, Iacoe E, Forman J, Polderman J, et al. 2022. Responding to the COVID-19 pandemic: Development of a critical care nursing surge model to meet patient needs and maximise competencies. Australian Critical Care, 35(1): 13–21.
Lawler PR, Goligher EC, Berger JS, Gong MN, Carrier M, Reynolds HR, et al. 2021. Therapeutic anticoagulation with heparin in noncritically ill patients with Covid-19. New England Journal of Medicine, 385(9): 790–802.
Lee J. 2021. Alberta rolls out its first outpatient COVID-19 treatment as experts warn it’s not a vaccine substitute [online]: Available from cbc.ca/news/canada/calgary/covid-alberta-treatment-drug-seniors-1.6243409#:∼:text=CBC%20News%20Loaded-,Alberta%20rolls%20out%20its%20first%20outpatient%20COVID%2D19%20treatment%20as,not%20a%20replacement%20for%20vaccination.
Letterio A. 2021. Nurses at Kamloops, B.C. hospital walking off job due to exhaustion. [online]: Available from globalnews.ca/news/8137390/kamloops-nurses-walking-off-job/.
Lief L, Berlin DA, Maciejewski RC, Westman L, Su A, Cooper ZR, et al. 2018. Dying Patient and Family Contributions to Nurse Distress in the ICU. Annals of the American Thoracic Society, 15(12): 1459–1464.
Litz BT, Stein N, Delaney E, Lebowitz L, Nash WP, Silva C, et al. 2009. Moral injury and moral repair in war veterans: a preliminary model and intervention strategy. Clinical Psychology Review, 29(8):695–706.
Liu X, Kakade M, Fuller CJ, Fan B, Fang Y, Kong J. et al. 2012. Depression after exposure to stressful events: lessons learned from the severe acute respiratory syndrome epidemic. Comprehensive Psychiatry, 53(1): 15–23.
Lung FW, Lu YC, Chang YY, Shu BC. Mental symptoms in different health professionals during the sars attack: A follow-up study. Psychiatr Q. 2009;80(2): 107–116.
Mahoney A, White RD, Velasquez A, Barrett TS, Clark RH, and Ahmad KA. 2020. Impact of restrictions on parental presence in neonatal intensive care units related to coronavirus disease 2019. Journal of Perinatology, 40(Suppl 1): 36–46.
Malik M, Peirce J, Wert MV, Wood C, Burhanullah H, and Swartz K. 2021. Psychological first aid well-being support rounds for frontline healthcare workers during COVID-19. Frontiers in Psychiatry 12: 669009.
Martillo MA, Dangayach NS, Tabacof L, Spielman LA, Dams-O’Connor K, Chan, CC. et al. 2019. Postintensive care syndrome in survivors of critical illness related to coronavirus disease 2019: Cohort study from a new york city critical care recovery clinic. Critical Care Medicine, 49(9): 1427–1438.
Maslach,C, Jackson, SE. 1981. The measurement of experienced burnout. Journal of Organizational Behavior, 2: 99–113.
Matava CT, Kovatsis PG, Lee JK, Lee JK, Castro P, Denning S. 2020. et al. Pediatric airway management in COVID-19 Patients: Consensus guidelines from the society for pediatric anesthesia’s pediatric difficult intubation collaborative and the Canadian pediatric anesthesia society. Anesthesia and Analgesia, 131(1): 61–73.
Matsuishi K, Kawazoe A, Imai H, Ito A, Mouri K, Kitamura N, et al. Psychological impact of the pandemic (H1N1) 2009 on general hospital workers in Kobe. Psychiatry Clin Neurosci. 2012;66(4): 353–360.
Maunder RG, Lancee WJ, Balderson KE, Bennett JP, Borgundvaag B, Evans S, et al. 2006. Long-term psychological and occupational effects of providing hospital healthcare during SARS outbreak. Emerging Infectious Diseases 12(12): 1924–1932.
Maunder RG, Lancee WJ, Rourke S, Hunter JJ, Goldbloom D, Balderson, K. et al. 2004. Factors associated with the psychological impact of severe acute respiratory syndrome on nurses and other hospital workers in Toronto. Psychosomatic Medicine, 66(6): 938–942.
Maves RC, Downar J, Dichter JR, Hick JL, Devereaux A, Geiling JA, et al. 2020. Triage of scarce critical care resources in COVID-19 an implementation guide for regional allocation: An Expert panel report of the task force for mass critical care and the American college of chest physicians. Chest, 158(1): 212–225.
Mayer KP, Boustany H, Cassity EP, Soper, MK, Kalema, AG, Hatton KJ, et al. ICU Recovery Clinic Attendance, Attrition, and Patient Outcomes: The Impact of Severity of Illness, Gender, and Rurality. Crit Care Explor. 2020;2(10):e0206.
Mayland CR, Harding AJE, Preston N, and Payne S. 2020. Supporting adults bereaved through COVID-19: A rapid review of the impact of previous pandemics on grief and bereavement. Journal of Pain and Symptom Management, 60(2): e33–e39.
McAlonan GM, Lee AM, Cheung V, Tsang KWT, Sham PC, Chua SE, et al. 2007. Immediate and sustained psychological impact of an emerging infectious disease outbreak on health care workers. Canadian Journal of Psychiatry. Revue Canadienne de Psychiatrie 52(4): 241–247.
McCarthy J, Deady R. 2008. Moral distress reconsidered. Nurs Ethics. 15(2): 254–262.
McCarthy, N. 2020. Forbes.
McGillivary K. 2021. CBC News. Low oxygen supplies due to COVID-19 force Michael Garron Hospital to transfer some patients. [online]: Available from cbc.ca/news/canada/toronto/oxygen-supplies-michael-garron-1.6007743.
McKendrick, D. 2021. Government of Canada to provide COVID-19 support to Manitoba. CTV News. [online]: Available from winnipeg.ctvnews.ca/government-of-canada-to-provide-covid-19-support-to-manitoba-1.5441182
McMahon M, Nadigel J, Thompson E, and Glazier RH. 2020. Informing Canada’s Health System Response to COVID-19: Priorities for Health Services and Policy Research. Healthcare Policy 16(1): 112–124.
Miller AG, Roberts KJ, Smith BJ, Burr KL, Hinkson CR, Hoerr CA, et al. 2021. Prevalence of Burnout Among Respiratory Therapists Amidst the COVID-19 Pandemic. Respiratory Care 16: 09283.
Mistraletti G, Giannini A, Gristina G, Malacarne P, Mazzon D, Cerutti E, et al. 2021. Why and how to open intensive care units to family visits during the pandemic. Critical Care 25(1): 191.
Mitchell R, Choi KB, Pelude L, Rudnick W, Thampi N, Taylor G. et al. 2021. Patients in hospital with laboratory-confirmed COVID-19 in a network of Canadian acute care hospitals, Mar. 1 to Aug. 31, 2020: a descriptive analysis. CMAJ Open 9(1): E149–E156.
Mitra AR, Fergusson NA, Lloyd-Smith E, Wormsbecker A, Foster D, Karpov A, et al. Baseline characteristics and outcomes of patients with COVID-19 admitted to intensive care units in Vancouver, Canada: a case series. CMAJ: Canadian Medical Association Journal, 192(26): E694E701.
Moore-Black, D. and Kevin MD. 2021. The moral destruction of ICU nurses.
Moriarty T, Boczula AE, Thind EK, Loreto N, McElhaney JE. 2021. Excess All-Cause Mortality During the COVID-19 Epidemic in Canada. Royal Society of Canada.
Munshi L, Odutayo A, Evans GA, Keresteci M, Drury J, Kain D, et al. 2021. (on behalf of the Ontario COVID-19 Science Advisory Table). Impact of Hospital Visitor Restrictions During the COVID-19 Pandemic, Science Table, COVID-19 Advisory Board for Ontario, Vol. 1.0.
Murthy S, Archambault PM, Atique A, Carrier FM, Cheng MP, Codan C, et al. 2021. Characteristics and outcomes of patients with COVID-19 admitted to hospital and intensive care in the first phase of the pandemic in Canada: a national cohort study. CMAJ Open 9(1): E181–E188.
Nadim MK, Forni LG, Mehta RL, Connor MJ, Liu KD, Ostermann M, et al. 2020. COVID-19-associated acute kidney injury: consensus report of the 25th Acute Disease Quality Initiative (ADQI) Workgroup. Nature Reviews Nephrology 16(12): 747–764.
National Institute for Care Excellence. 2018. Chapter 39: Bed Occupancy: Emergency and acute medical care in over 16’s. Service Delivery and organisation. NICE Guideline 94. [online]: Available from nice.org.uk/guidance/ng94/evidence/39.bed-occupancy-pdf-172397464704.
Nickell LA, Crighton EJ, Tracy CS, Al-Enazy H, Bolaji Y, Hanjrah S, et al. 2004. Psychosocial effects of SARS on hospital staff: Survey of a large tertiary care institution. CMAJ: Canadian Medical Association Journal 170(5): 793–798.
Oakley C, Pascoe C, Balthazor D, Bennett D, Gautam N, Isaac J, et al. 2020. Assembly Line ICU: what the Long Shops taught us about managing surge capacity for COVID-19. BMJ Open Quality 9(4): e001117.
Ontario Science Table. 2022. Current COVID-19 Risk in Ontario by Vaccination Status. [online]: Available from covid19-sciencetable.ca/wp-content/uploads/2022/02/2022-02-03-Current-COVID-19-Risk-in-Ontario-by-Vaccination-Status.png
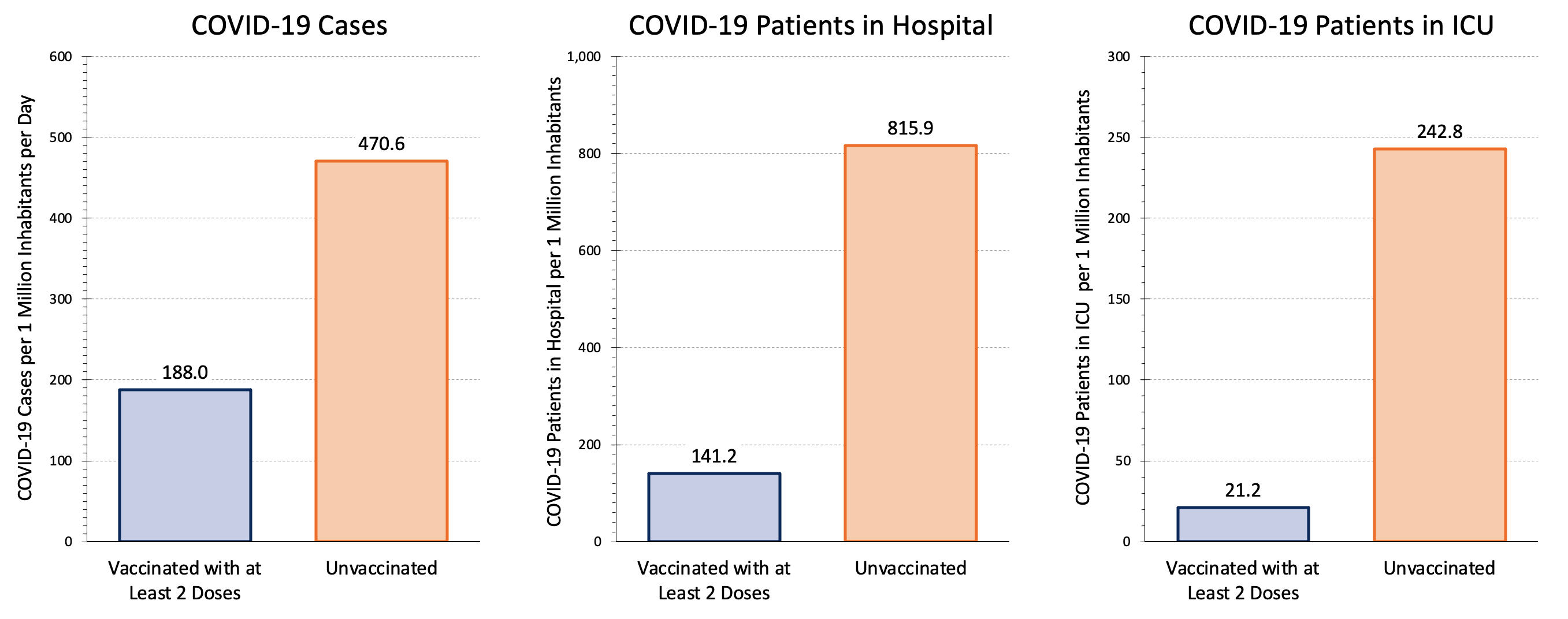{kind=link}
Organisation for Economic Co-operation and Development. 2021. Health at a Glance 2021: OECD Indicators. [online]: Available from oecd-ilibrary.org/sites/e5a80353-en/index.html?itemId=/content/component/e5a80353-en
Organisation for Economic Co-operation and Development. 2021. [online]: Available from read.oecd-ilibrary.org/social-issues-migration-health/health-at-a-glance-2021_e5a80353-en#page1.
Ozawa M, Sakaki H, Meng X. 2021. Family Presence Restrictions and Telemedicine Use in Neonatal Intensive Care Units during the Coronavirus Disease Pandemic. Children 8(7): 590.
Pan H, Peto R, Henao-Restrepo AM, Preziosi M-P, Sathiyamoorthy V, Karim QA, et al. 2021. Repurposed antiviral drugs for Covid-19 – Interim WHO solidarity trial results. New England Journal of Medicine 384(6): 497–511.
Papazoglou K, and Chopko B. 2017. The Role of Moral Suffering (Moral Distress and Moral Injury) in Police Compassion Fatigue and PTSD: An Unexplored Topic. Frontiers in Psychology 8: 1999.
Parhar KKS, Lequier L, Blackwood J, Zuege DJ, Singh G. 2020. Optimizing provision of extracorporeal life support during the COVID-19 pandemic: practical considerations for Canadian jurisdictions. CMAJ : Canadian Medical Association Journal 192: E372–E374.
Pearson H. 2020. COVID-19: Staff at Calgary hospitals told to ‘engage in oxygen conservation’ as cases rise, Global News. [online]: Available from globalnews.ca/news/7492963/coronavirus-calgary-hospitals-oxygen-conservation/
Pelosi P, Ball L, Barbas CSV, Bellomo R, Burns KEA, Einav S, et al. 2021. Personalized mechanical ventilation in acute respiratory distress syndrome. Critical Care 25(1): 250.
Penque S. 2019. Mindfulness to promote nurses’ well-being. Nurs Manage. 50(5): 38–44.
Petrinec AB, Martin BR. 2018. Post-intensive care syndrome symptoms and health-related quality of life in family decision-makers of critically ill patients. Palliat Support Care. 16(6): 719–724.
Plouffe RA, Nazarov A, Forchuk CA, Gargala D, Deda E, Le T, et al. 2021. Impacts of morally distressing experiences on the mental health of Canadian health care workers during the COVID-19 pandemic. European Journal of Psychotraumatology 12(1): 1984667.
Preti E, Di Mattei V, Perego G, Ferrari F, Mazzetti M, Taranto P, et al. 2020. The psychological impact of epidemic and pandemic outbreaks on healthcare workers: Rapid review of the evidence. Curr Psychiatry Rep. 22(8): 43.
Public Health Agency of Canada. 2022. Detailed preliminary information on cases of COVID-19, 2020-2022: 6-Dimensions (Aggregated data).
Pun BT, Badenes R, Heras La Calle G, Orun OM, Chen W, Raman R, et al. 2021. Prevalence and risk factors for delirium in critically ill patients with COVID-19 (COVID-D): A multicentre cohort study Respir Med. Lancet, 9(3): 239–250.
Rae PJL, Pearce S, Greaves PJ, Dall’Ora C, Griffiths P, and Endacott R. 2021. Outcomes sensitive to critical care nurse staffing levels: A systematic review. Intensive Crit Care Nurs. 67: 103110.
Ramanathan K, Shekar K, Ling RR, Barbaro RP, Wong SN, Tan CS, et al. 2021. Extracorporeal membrane oxygenation for COVID-19: a systematic review and meta-analysis. Critical Care 25(1): 211.
Rawal G, Yadav S, Kumar R. 2017. Post-intensive care syndrome: An overview. Journal of Translational Internal Medicine 5(2): 90–92.
REMAP-CAP Investigators. 2021. Interleukin-6 Receptor Antagonists in Critically III Patients with Covid-19. N Engl J Med. Apr 22;384(16): 1491–1502.
Remy KE, Verhoef PA, Malone JR, Ruppe MD, Kaselitz TB, Lodeserto F, et al. 2020. Caring for critically III adults with coronavirus disease 2019 in a PICU: Recommendations by dual trained intensivists. Pediatr Crit Care Med. Jul;21(7): 607–619.
Resick PA, Monson CM, and Chard KM. 2017. Cognitive Processing Therapy for PTSD. Guilford Press. New York.
Rieger S. 2020. Calgary hospitals told to conserve oxygen, but doctors fear request is a red flagCBC News. [online]: Available from cbc.ca/news/canada/calgary/oxygen-delivery-alberta-hospitals-covid-19-1.5822825.
Rieger, S. 2021. Alberta asks Ottawa for help to airlift COVID-19 patients out of the province. CBC news. [online]: Available from cbc.ca/news/canada/calgary/alberta-asks-ottawa-for-covid-19-help-1.6184484
Rinaldi L. 2021. We have 28 people waiting for a bed”: Q&A with Michael Warner, the Toronto doctor who’s gone viral sharing his patients’ stories. Toronto Life. [online]: Available from torontolife.com/city/nearly-all-of-my-patients-are-essential-workers-or-related-to-one-and-we-have-28-more-people-waiting-for-an-icu-bed-a-qa-with-michael-warner-the-toronto-icu-director-whos-gone-viral-s/
Robert R, Kentish-Barnes N, Boyer A, Laurent A, Azoulay E, and Reignier J, et al. 2020. Ethical dilemmas due to the Covid-19 pandemic. Annals of Intensive Care 10(1): 84.
Rodriguez-Morales AJ, Cardona-Ospina JA, Gutiérrez-Ocampo E, Gutiérrez-Ocampo E, Villamizar-Peña R, and Holguin-Rivera Y, et al. 2020. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Medicine and Infectious Disease 34: 101623.
Rose L, Goldsworthy S, O’Brien-Pallas L, and Nelson S. 2008. Critical care nursing education and practice in Canada and Australia: a comparative review. Int J Nurs Stud. 45(7): 1103–1109.
Rousseau AF, Prescott HC, Brett SJ, Weiss B, Azoulay E, Creteur J, et al. 2021. Long-term outcomes after critical illness: Recent insights. Critical Care 25(1):108.
Royal College of Physicians and Surgeons of Canada. 2019. Pathway to Competence: General Pediatrics. [online]: Available from royalcollege.ca/rcsite/ibd-search-e.
Rush University. 2020. This is what Rush was built for.
Sabeti F, Mohammadpour M, Pouraboli B, Tahmasebi M, Hasanpour M. 2021. Health care providers’ experiences of the non-pharmacological pain and anxiety management and its barriers in the pediatric intensive care units. J Pediatr Nurs. 60: e110–e116.
Sander LB, Schorndanner J, Terhorst Y, Spanhel K, Pryss R, Baumeister H, and Messner EM. 2020. Help for trauma from the app stores?' A systematic review and standardised rating of apps for Post-Traumatic Stress Disorder (PTSD). European Journal of Psychotraumatology 11(1): 1701788.
Scales D. 2020. An understaffed hospital battles COVID-19. Health Aff (Millwood). 39(8): 1450–1452.
Schneider BC, Schneider SP. 2020. ICU buddy staffing to combat COVID-19. Nurs Manage. 51(10): 36–42.
Schwartz I, Lee TC, McDonald EG, Laupland K. 2021. What went wrong: A reckoning of Canada’s contributions to evidence-based medicine through clinical trials during the COVID-19 pandemic. Journal of the Association of Medical Microbiology Canada,
Science Table. 2021. COVID-19 Advisory for Ontario. [online]: Available from covid19-sciencetable.ca/sciencebrief/#infectious-diseases-clinical-care
Sheikh A, Kerr S, Woolhouse M, McMenamin J, Robertson C and EAVE II Collaborators. 2022. Severity of omicron variant of concern and effectiveness of vaccine boosters against symptomatic disease in Scotland (EAVE II): a national cohort study with nested test-negative design. Lancet Infectious Diseases
Shekerdemian LS, Mahmood NR, Wolfe KK, Riggs BJ, Ross CE, McKiernan CA, et al. 2020. Characteristics and Outcomes of Children With Coronavirus Disease 2019 (COVID-19) Infection Admitted to US and Canadian Pediatric Intensive Care Units. JAMA Pediatr. 174(9): 868–873.
Silas L, and Smith H. 2021. Opinion: Nurse staffing crisis calls for better national planning. Edmonton Journal. [online]: Available from edmontonjournal.com/opinion/columnists/opinion-nurse-staffing-crisis-calls-for-better-national-planning.
Simone R. 2021. 4 Post-Pandemic Healthcare Construction Trends. Healthcare Facilities Today. [online]: Available from healthcarefacilitiestoday.com/posts/4-Post-Pandemic-Healthcare-Construction-Trends--26434.
Simone R. 2020. COVID-19’s Impact on Healthcare Design and Construction. Healthcare Construction and Operations. [online]: Available from hconews.com/2020/09/15/covid-19s-impact-on-healthcare-design-and-construction/.
Singh J, Green MB, Lindblom S, Reif MS, Thakkar NP, and Papali A. 2021. Telecritical Care Clinical and Operational Strategies in Response to COVID-19. Telemedicine Journal and e-Health 27(3):261–268.
Sinha R, Aramburo A, Deep A, Bould E-J, Buckley HL, Draper ES, et al. 2021. Caring for critically ill adults in paediatric intensive care units in England during the COVID-19 pandemic: planning, implementation and lessons for the future. Archives of Disease in Childhood 106(6): 548–557.
Skipper CP, Pastick KA, Engen NW, Bould E-J, Buckley HL, Draper ES, et al. 2020. Hydroxychloroquine in nonhospitalized adults with early COVID-19: A randomized trial. Ann Intern Med.
Smetanin P, Stiff D, Kumar A, Kobak P, Zarychanski R, Simonsen N, et al. 2009. Potential intensive care unit ventilator demand/capacity mismatch due to novel swine-origin H1N1 in Canada. The Canadian Journal of Infectious Diseases 20(4): e115–e123.
Statista. 2021. Health, Pharma and Medtech: State of Health. Number of COVID-19 deaths in Canada by age. [online]: Available from statista.com/statistics/1228632/number-covid-deaths-canada-by-age/.
Statista. 2020. Rates of intensive care beds in hospitals in select countries worldwide as of 2020. [online]: Available from statista.com/statistics/1115999/intensive-care-bed-rates-hospitals-select-countries-worldwide/
Statistics Canada. Table 13-10-0774-01 Detailed preliminary information on cases of COVID-19, 2020-2021: 6-Dimensions (Aggregated data), Public Health Agency of Canada https://doi.org/10.25318/1310077401-eng Accessed October 23, 2021.
Stelfox HT, Hemmelgarn BR, Bagshaw SM, Gao S, Doig CJ, Nijssen-Jordan C, et al. 2012. Intensive care unit bed availability and outcomes for hospitalized patients with sudden clinical deterioration. Arch Intern Med 172: 467–74.
Stiff D, Kumar A, Kissoon N, Fowler R; Jouvet P, Skippen P, et al. 2011. Potential pediatric intensive care unit demand/capacity mismatch due to novel pH1N1 in Canada. Pediatr Crit Care Med. 12(2): e51–e57.
Tardif JC, Bouabdallaoui N, L’Allier PL, Gaudet D, Shah B, Pillinger MH, et al. 2021. Colchicine for community-treated patients with COVID-19 (COLCORONA): a phase 3, randomised, double-blinded, adaptive, placebo-controlled, multicentre trial. Lancet Respir Med. 9(8): 924–32.
Teixeira C, and Rosa RG. 2018. Post-intensive care outpatient clinic: is it feasible and effective? A literature review. Ambulatório pós-unidade de terapia intensiva: é viável e efetivo? Uma revisão da literatura. Revista Brasileira de Terapia Intensiva 30(1):98–111.
The SARS Commission. 2007. [online]: Available from archives.gov.on.ca/en/e_records/sars/report/v1.html.
Tierney LT, and Conroy KM. 2014. Optimal occupancy in the ICU: a literature review. Aust Crit Care. 27(2): 77–84.
Tobin MJ, Laghi F, Jubran A. 2020. Why COVID-19 Silent Hypoxemia Is Baffling to Physicians. American Journal of Respiratory and Critical Care Medicine 202(3): 356–360.
Tomblin-Murphy G, Sampalli T, Bearskin LB, Cashen N, Cummings G, Rose AE, et al. 2022. Investing in Canada’s nursing workforce post-pandemic: A call to action. Royal Society of Canada. [online]: Available from docs.google.com/viewer?url=https%3A%2F%2Frsc-src.ca%2Fsites%2Fdefault%2Ffiles%2Fpdf%2FNursing%2520PB_Preprint%2520ES_4.pdf
Tran DT, Thanh NX, Opgenorth D, Wang X, Zuege D, Zygun DA, et al. 2019. Association between strained ICU capacity and healthcare costs in Canada: A population-based cohort study. J Crit Care. 51: 175–183.
Tsang JLY, Fowler R, Cook DJ, Ma H, and Binnie A. 2021. How can we increase participation in pandemic research in Canada? Can J Anesth/J Can Anesth.
Ulloa AC, Buchan SA, Daneman N, and Brown KA. 2022. Estimates of SARS-CoV-2 omicron variant severity in Ontario, Canada. JAMA.
University Health Network 2022.
Uppal A, Silvestri DM, Siegler M, Natsui S, Boudourakis L, Salway RJ, et al. 2020. Critical care and emergency department response at the epicenter of the COVID-19 pandemic. Health Aff (Millwood). 39(8): 1443–1449.
Valiani S, Terrett L, Gebhardt C, Prokopchuk-Gauk O, Isinger M. 2020. Development of a framework for critical care resource allocation for the COVID-19 pandemic in Saskatchewan. CMAJ: Canadian Medical Association Journal, 192(37): E1067–E1073.
Vescera Z. 2021. Sask. prepares to send ICU patients to Ontario as COVID-19 crushes hospitals. Saskatoon Star Phoenix. [online]: Available from thestarphoenix.com/news/saskatchewan/sask-prepares-to-send-icu-patients-to-ontario-as-covid-19-crushes-hospitals.
Warncke G, Hoffmann F, Sasse M, Singer G, Szilagyi I, Till H, et al. 2018. A multinational survey on the infrastructural quality of paediatric intensive care units. Annals of Intensive Care 8(1): 105.
Weeks C. 2022. Most provinces’ stockpiles of ‘critical’ COVID-19 drug Paxlovid sitting unused during sixth wave. The Globe and Mail. [online]: Available from theglobeandmail.com/canada/article-covid-19-antiviral-drug-paxlovid-being-dispensed-at-low-rates-across/
Weil MH, and Tang W. 2011. From intensive care to critical care medicine: a historical perspective. American Journal of Respiratory and Critical Care Medicine 183(11): 1451–1453.
West AJ, Nickerson J, Breau G, Mai P, and Dolgowicz C. 2016. Staffing patterns of respiratory therapists in critical care units of Canadian teaching hospitals. Canadian Journal of Respiratory Therapy 52: 75–80.
West A. 2021. Respiratory Therapy in Canada/Confronting Covid-19. AARC. aarc.org/an21
Wilcox ME, Harrison D, Patel A, Patel A, and Rowan K. 2020. Higher ICU Capacity Strain Is Associated with Increased Acute Mortality in Closed ICUs, Critical Care Medicine. 48: 709–716
Wilkerson RG, Adler JD, Shah NG, and Brown R. 2020. Silent hypoxia: A harbinger of clinical deterioration in patients with COVID-19. Am J Emerg Med. 38(10): 2243.e5–2243.e6.
Williams GA, Maier CB, Scarpetti G, Belvis AG, Fattore G, Morsella A, Pastorino G. et al. 2020. What strategies are countries using to expand health workforce surge capacity during the COVID-19 pandemic? Eurohealth, 26(2): 51–57.
Winkelmann J, Webb E, Williams GA, Hernández-Quevedo C, Maier CB, and Panteli D. 2021. European countries’ responses in ensuring sufficient physical infrastructure and workforce capacity during the first COVID-19 wave. Health Policy,
Wittnebel, J. 2021. Standard of care can no longer be met’: Infection surge creates ‘desperate’ scenario for hospitals. The Pointer. [online]: Available from thepointer.com/article/2021-04-12/standard-of-care-can-no-longer-be-met-infection-surge-creates-desperate-scenario-for-hospitals.
Wong J. 2022. Missed diagnoses, PPE failures: How the Misericordia COVID-19 outbreak unfolded. [online]: Available from cbc.ca/news/canada/edmonton/misericordia-covid19-outbreak-report-1.6284068.
Wong TW, Yau JK, Chan CL, Cecilia LWK, Rosalie SY, Ho SMY, et al. 2005. The psychological impact of severe acute respiratory syndrome outbreak on healthcare workers in emergency departments and how they cope. Eur J Emerg Med. 12(1):13–18.
World Health Organization. 2020. Regional Office for Europe. Strengthening the health system response to COVID-19: technical guidance #1: maintaining the delivery of essential health care services while mobilizing the health workforce for the COVID-19 response. World Health Organization. Regional Office for Europe. [online]: Available from apps.who.int/iris/handle/10665/332559.
Wynne R, Davidson PM, Duffield C, Jackson D, and Ferguson C. 2021. Workforce management and patient outcomes in the intensive care unit during the COVID-19 pandemic and beyond: a discursive paper. J Clin Nurs.
Yang SS, Lipes J, Dial S, Schwartz B, Laporta D, Wong E, Baldry C, et al. 2020. Outcomes and clinical practice in patients with COVID-19 admitted to the intensive care unit in Montréal, Canada: a descriptive analysis. CMAJ Open 8(4): E788–E795.
Appendix A Moral Suffering includes Moral Distress and Moral Injury
Moral distress is described as involving a threat to one’s moral integrity. Moral integrity is the sense of wholeness and self-worth that comes from having clearly defined values that are congruent with one’s actions and perceptions (Hardingham 2004). McCarthy and Deady (2008); Epstein et al. (2020) reported moral distress may be pervasive among caregiving professionals who are expected to make decisions and judgments that encompass moral components during complex incidents. Caution should be used to differentiate moral distress from emotional distress experienced by care providers working within a stressful environment or with a challenging patient case, without the essential ethical component of moral distress.
Moral Injury is described as act of transgression that creates dissonance and conflict because it violates assumptions and beliefs about right and wrong and personal goodness (Litz et al. 2009).
Compassion Fatigue: This is defined as a secondary traumatic stress that results from frontline professionals “cost of caring” (Figley 2002). Compassion fatigue is cognitively related to moral suffering experienced by first responders in the line of duty and continuous experience of multiple critical incidents leads to the experience of moral distress, moral injury, and compassion fatigue, which may in turn increase vulnerability to PTSD symptomatology (Papazoglou and chopko 2017; Clay 2021).
Burnout: Health care worker burnout has been defined as a reaction to chronic stress marked by emotional exhaustion, depersonalization, and low sense of personal accomplishment (Maslach and Jackson 1981; Howell 2021). Recent theories have proposed that health care workers burnout is a manifestation of moral injury. This is the challenge of simultaneously knowing what care patients need but being unable to provide it due to constraints that are beyond our control (Dean et al. 2019). According to Litz (2009), moral injury reflects the psychosocial, behavioural, and even spiritual impacts of “failing to prevent or bearing witness to acts that transgress deeply held moral beliefs and expectations”.
Post-Traumatic Stress Disorder: The American Psychiatric Association defines PTSD as a disorder in individuals exposed, directly or indirectly to a traumatic event, like death threat, serious injury, and or sexual violence. Preti et al. (2020) reviewed 23 studies that showed that during an outbreak, 52 percent of health care workers scored above the threshold for a PTSD diagnosis.
Information & Authors
Information
Published In

FACETS
Volume 7 • Number 1 • January 2022
Pages: 1411 - 1472
Editor: Russel MacDonald
History
Received: 1 February 2022
Accepted: 24 June 2022
Version of record online: 1 December 2022
Notes
This paper is part of the Royal Society of Canada’s COVID-19 Task Force Collection.
Copyright
© 2022 Gibney et al. This work is licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Key Words
- COVID-19
- critical care
- pediatric intensive care
- intensive care units
- public health
- critical care nursing
- respiratory therapy
- mechanical ventilation
- extracorporeal lung support
- acute respiratory distress syndrome
- long-COVID
- hospital capacity
- triage protocol
- post intensive care syndrome
- post-traumatic stress syndrome
- critical care research
- hospital construction
Sections
Subjects
Authors
Author Contributions
RTNG and SM conceived and designed the study.
CB, MG, EF, RF, CJ, RJK, KM, TM, BP, and TT performed the experiments/collected the data.
CB, MG, EF, RF, CJ, RJK, KM, TM, BP, and TT analyzed and interpreted the data.
CB, MG, EF, RF, CJ, RJK, KM, TM, BP, and TT contributed resources.
CB, MG, EF, RF, CJ, RJK, KM, TM, BP, and TT drafted or revised the manuscript.
Metrics & Citations
Metrics
Other Metrics
Citations
Cite As
R.T. Noel Gibney, Cynthia Blackman, Melanie Gauthier, Eddy Fan, Robert Fowler, Curtis Johnston, R. Jeremy Katulka, Samuel Marcushamer, Kusum Menon, Tracey Miller, Bojan Paunovic, and Teddie Tanguay. 2022. COVID-19 pandemic: the impact on Canada’s intensive care units. FACETS.
7: 1411-1472.
https://doi.org/10.1139/facets-2022-0023
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
Cited by
1. Derivation and Validation of a Point-based Forecasting Tool for SARS-CoV-2 Critical Care Occupancy
2.
3. Delayed Access to Medical Care and Psychological Distress among Chinese Immigrants in Canada during the Pandemic
4. COVID-19 in a rural intensive care unit in Northern British Columbia: Descriptive analysis of outcomes and demands on rural resources
5. The Greatest Challenges of Pediatric Critical Care Pulmonology in the After-COVID Era: A Narrative Review
6. Delivery and Prioritization of Surgical Care in Canada During COVID-19: An Environmental Scan
7. The Role of Canadian respiratory therapists in adult critical care (ICURT-CAN): A scoping review
8. SARS-CoV-2, COVID-19, and Children: Myths and Evidence