Royal Society of Canada working group on health research system recovery: strengthening Canada’s health research system after the COVID-19 pandemic
Abstract
The Royal Society of Canada Working Group on Health Research System Recovery developed actionable recommendations for organizations to implement to strengthen Canada’s health research system. Recommendations were based on input from participants from G7 countries and Australia and New Zealand. Participants included health research funding agency leaders; research institute leaders; health, public health, and social care policy-makers; researchers; and members of the public. The recommendations were categorized using the World Health Organization’s framework for health research systems and include governance/stewardship: (1) Outline research logistics as part of emergency preparedness to streamline research in future pandemics. (2) Embed equity and inclusion in all research processes. (3) Facilitate streamlined, inclusive, and rigorous processes for grant application preparation and review. (4) Create knowledge mobilization infrastructure to support the generation and use of evidence. (5) Coordinate research efforts across local, provincial, national, and international entities. Financing: (6) Reimagine the funding of health research. Capacity building: (7) Invest in formative training opportunities rooted in equity, diversity, and anti-racism. (8) Support researchers’ career development throughout their career span. (9) Support early career researchers to establish themselves. Producing and using research: (10) Strengthen Indigenous health research and break down systemic barriers to its conduct. (11) Develop mechanisms to produce novel research. (12) Enhance research use across the health research ecosystem.
Introduction
The COVID-19 pandemic tested health research systems (Hanney et al. 2022). The pandemic also produced rapid and substantial changes in research conduct and in how research funders and researchers function, including their engagement with policy-makers (anyone responsible for developing and implementing policies at organizational, local, provincial, or national levels) and other knowledge users (e.g., patients/people with lived experience, other members of the public, and clinicians). Although rapid research and evidence use took place, the pandemic also revealed gaps and inefficiencies in the health research system. In response, the Royal Society of Canada Working Group on Health Research System Recovery conducted an international initiative that included a series of knowledge exchange sessions and surveys. The purpose of this initiative was to develop actionable recommendations that a range of organizations can act on, individually and collectively, to strengthen Canada’s health research system after the pandemic in the short, medium, and long term. This initiative was carried out through a partnership between the Royal Society of Canada, the Canadian Institutes of Health Research (CIHR), Health Research BC, and the Knowledge Translation Program at St. Michael’s Hospital.
The intended population of participants in this initiative consisted of leadership (e.g., presidents, vice-presidents, and management) from health research funding agencies in the G7 countries, as well as Australia and New Zealand; health, public health, and social care policy-makers from these countries; leadership from research institutes in these countries; and members of the public and researchers from Canada. These sessions and surveys were structured around the four functions of the World Health Organization (WHO) framework for health research systems: (1) governance/stewardship, including vision, priority setting, ethics, and monitoring/evaluation; (2) financing; (3) capacity building, which encompasses capacity to conduct (including supporting the life cycle of the researcher), receive, and use research; and (4) producing and using research to improve health and strengthen the public, social, and health care systems (see Appendix A for definitions) (Pang et al. 2003).
Of note, when this initiative was launched, the co-chairs (Drs. Clifford, Holmes, and Straus) held meetings with the Scientific Director of CIHR’s Institute of Indigenous Peoples’ Health, who agreed to lead a parallel process focusing on Indigenous peoples’ priorities for changing the health research ecosystem. Because of leadership changes within that institute, the parallel process has not been undertaken at the time of writing this report. As such, although some Indigenous individuals participated in the surveys and knowledge exchange sessions described here and although suggestions related to Indigenous health research were identified, this process was not led by Indigenous individuals. The suggestions related to Indigenous health research, which point to certain systemic changes that would facilitate Indigenous-led research, are included in this report and will be provided to the Institute of Indigenous Peoples’ Health for their information.
Methods
We used qualitative and quantitative methods, including surveys and knowledge exchange sessions, to develop recommendations to strengthen Canada’s health research ecosystem. From the sessions and surveys, we developed actions to accompany each recommendation to support the implementation of the recommendations.
Knowledge exchange sessions
Recruitment
We conducted three knowledge exchange sessions. For session 1, we purposefully recruited leadership from health research funding agencies as well as health, public health, and social care policy-makers in G7 countries, as well as Australia and New Zealand. For session 2, we purposefully recruited leadership from research institutes in G7 countries, as well as Australia and New Zealand. For sessions 1 and 2, participants were also recruited through the study team’s and project partners’ circles of contact and through snowball sampling via other participants. For session 3, we recruited members of the public and researchers living in Canada through the study team’s and project partners’ circles of contact, social media, and newsletters. Session 3 participants were sampled to reflect diversity across research areas and career stages (for researchers) and across gender, race, age, and geographic locations (for researchers and members of the public). This project was approved by the Unity Health Toronto Research Ethics Board. The discussion guide for each knowledge exchange session was co-created by researchers and knowledge users. See Appendix B for the session 1 discussion guide as an example. The guides for sessions 2 and 3 were developed iteratively, using the data from previous sessions. Prior to each knowledge exchange session, the guide was tested with two to three knowledge users and refined as needed to ensure clarity.
Data collection
We conducted three 3 h knowledge exchange sessions via video/teleconference: on 21 October 2022 (session 1), with leadership from health research funding agencies and health, public health, and social care policy-makers; on 26 October 2022 (session 2), with leadership from research institutes; and on 27 January 2023 (session 3), with members of the public and researchers. Sessions were held in English with provision of French interpretation when needed. The sessions were audio-recorded and transcribed. The sessions included small-group discussions (i.e., six–eight participants) to provide opportunities for all participants to share and large-group discussions (i.e., all session participants) to facilitate knowledge exchange among all participants. Discussions were guided by a member of the study team using a semi-structured discussion guide. We collected demographic data (e.g., gender and race) for only session 3 participants to sample to reflect diversity across these factors. We did not collect these data for sessions 1 and 2 participants as we purposefully recruited those in leadership positions and relevant policy-makers.
In sessions 1 and 2, we asked the leaders from health research funding agencies, research institutes, and policy-makers about what they did during the pandemic in terms of each of the four functions of the WHO health research system framework (Pang et al. 2003), what they plan to do in the future, and what they wish they had done differently. We prompted participants with additional questions situated in the framework, about how equity, diversity, inclusion, and anti-racism were considered across all of the activities; about sustaining, scaling, and spreading positive changes; about centralizing research priority setting; and about balancing COVID-19 and non-COVID-19 research.
At session 3, we asked members of the public and researchers what they thought research funders, policy-makers, and researchers should do in the future. We prompted participants with additional questions situated in the framework (Pang et al. 2003), about how equity, diversity, inclusion, and anti-racism could be better integrated into Canada’s health research system; about how to reduce barriers to involving patients and members of the public in health research; about how to sustain a health research workforce; and about how to balance COVID-19 and non-COVID-19 research in future health or public health emergencies.
Analysis
Transcripts were generated from the small- and large-group discussions at each of the sessions, for a total of 13 transcripts. Two experienced researchers double coded 15% of the transcripts. They discussed and resolved discrepancies where kappa was less than 0.6. Data were analyzed using a framework rapid analysis approach (Hamilton 2013; Gale et al. 2019).
Surveys
Recruitment and data collection
Three surveys were disseminated. The surveys were co-created by the research team, which included knowledge users. See Appendix C for the surveys. The surveys were reviewed by three to five knowledge users prior to dissemination to assess face validity and to ensure the surveys were not onerous to complete. The Total Design Method (Hoddinott and Bass 1986) was used to create and deliver survey reminders. Survey 1 collected information about organizations’ strategies to support post-pandemic recovery of the health research ecosystem. Before the knowledge exchange sessions, this survey was sent to those who had agreed to participate in sessions 1 and 2 and was more broadly disseminated to representatives of related organizations (e.g., funding agencies) by email and social media. Survey respondents were asked whether they were implementing strategies within their organization to address any of the four functions of the WHO health research system framework (Pang et al. 2003) and whether the strategies had been modified to support post-pandemic recovery. The survey was available from 16 August to 14 October 2022, in both English and French.
Survey 2 was disseminated after the three knowledge exchange sessions. This survey was used to obtain feedback on the draft recommendations by asking participants to rate each recommendation in terms of its importance for implementation in Canada and to provide comments or suggestions on the recommendations. The survey was widely disseminated to all session participants, project partners, various relevant research funding agencies, research institutes, health organizations, and patient partner organizations, and was also distributed by social media in Canada. The survey was available from 24 April to 11 July 2023, in both English and French.
Survey 3 was used to prioritize implementation of actions that accompany the updated recommendations and to specify who should be responsible for implementing these tasks (e.g., Health Canada, CIHR, provincial/territorial governments, universities, other). The survey was widely disseminated to all session participants, project partners, various research funding agencies, research institutes, health organizations, and patient partner organizations, as well as by social media. The survey was available from 2 October to 18 October 2023, in both English and French.
Analysis
Across all three surveys, we analyzed categorical data using descriptive statistics and open-ended data using a framework rapid analysis approach (Hamilton 2013; Gale et al. 2019).
Note that this research is the result of these knowledge exchange sessions and surveys; it does not necessarily represent the views of the authors or their institutions.
Results
All knowledge exchange sessions and surveys were planned for the period August 2022 to October 2023. Results from each activity informed subsequent activities; as such, the findings from the sessions and surveys are presented sequentially.
Survey 1
A total of 42 individuals completed survey 1. Not all questions were answered by all participants, because the survey used branching to guide participant responses, and participants were not required to answer all questions. Therefore, numbers may not sum to 42 within some categories. Participants represented 40 organizations, including research organizations (50%, n = 20), health research funding agencies (23%, n = 9), research user organizations such as journals (13%, n = 5), advocacy organizations (13%, n = 5), and research consultant organizations (3%, n = 1). Participants represented six countries, with the majority from Canada (81%, n = 34). Other participants were from the United Kingdom (7%, n = 3), the United States (5%, n = 2), Germany (2%, n = 1), New Zealand (2%, n = 1), and the Netherlands (2%, n = 1).
Respondent organizations reported having modified their research processes in a number of ways in response to COVID-19. These approaches are summarized in Table 1, organized according to the four functions of the WHO health research system framework (Pang et al. 2003). The modifications tended to refocus organizational goals, projects, funding, and staff time toward COVID-19 and to developing capacity-building and knowledge mobilization events and materials specific to COVID-19.
Table 1.
| Function 1—governance/stewardship | Function 2—financing | Function 3—capacity building | Function 4—producing and using research |
|---|---|---|---|
• Identified and incorporated key COVID-19-related goals and priorities into organizational plans • Developed new projects and programs to study the impacts of COVID-19 • Created new teams and linkages, both internal and external to the organization • Implemented virtual processes (e.g., peer review meetings) to replace in-person processes • Put new or increased organizational focus on health equity | • Increased funding amount for COVID-19 research • Increased accessibility of funding for COVID-19 research to a broader applicant pool beyond researchers • Changed priorities of funded research to focus on COVID-19 recovery and broader, long-term impacts of COVID-19 • Tracked COVID-19 research funding allocation and needs | • Developed infrastructure and staff positions to support COVID-19 recovery • Supported staff and researchers according to their needs • Modified format and timelines of capacity-building programs • Downsized non-COVID-19 research to support other COVID-19 efforts | • Held COVID-19-related knowledge mobilization events for various audiences • Developed COVID-19-related knowledge mobilization materials • Supported partnerships and integrated knowledge mobilization activities • Modified formats of knowledge mobilization events • Developed new methods to share data (e.g., post publicly when preprints become available in registries) • Focused attention on equity, diversity, inclusion, and anti-racism in knowledge mobilization activities |
Knowledge exchange session 1
Leadership from health research funding agencies and health, public health, and social care policy-makers attended session 1. Ten individuals, representing nine organizations, participated in this session. The 10 participants represented organizations in Canada (70%, n = 7), the United Kingdom (10%, n = 1), Australia (10%, n = 1), and the United States (10%, n = 1). Most participants were leaders from health research funding agencies (70%, n = 7), two were policy-makers (20%), and one was a researcher (10%). All participants spoke English. Tables 2–5 summarize key themes related to what participants did, what they plan to do in the future, and what they wish they had done differently across each of the four functions of the WHO health research system framework (Pang et al. 2003).
Table 2.
| Topic | Participant responses |
|---|---|
| What participants did in this area | • Focused on the public health response and prevention (e.g., vaccine development and distribution), including funding for relevant COVID-19 research, as well as research relevant to future pandemics and natural disasters. • Moved governance committee meetings to virtual platforms. • Did not develop COVID-19-specific funding, focusing instead on a more holistic approach related to comorbidity and multi-morbidity impacts on health. • Developed joint research projects across organizations such as universities, clinical programs, provincial and territorial funders, and federal funders, increasing project coordination among researchers, clinicians, and government. |
| What participants plan to do in the future in this area | • Engage in more international research initiatives. • Focus on investigating “long COVID”. • Continue virtual and hybrid models for various meetings (e.g., internal meetings, knowledge exchange events, conferences, peer review meetings, capacity-building sessions). • Maintain the responsive and flexible research administrative infrastructure that was developed during the COVID-19 pandemic, in preparation for future global health crises. |
| What participants wish they had done differently in this area | • Change should be initiated by the health care system to integrate research ecosystem changes. This could promote further alignment and collaboration between clinical settings and researchers by increasing health care decision-makers access to researchers. • Have a unified agenda for public and private funders in the health research ecosystem, and increase funding transparency and coordination to minimize duplication while facilitating replication. • Each province/territory should have a strategic research advisory committee, with pan-Canadian linkages. • Find efficiencies in the processes for research ethics and contract approvals (e.g., centralize processes) across regions/provinces/territories, to reduce delays. • Address the gaps in infrastructure that emerged during the pandemic, particularly related to research infrastructure capacity and clinical trial readiness such as cross-institutional and cross-jurisdictional contracts. • Improve clinical trial readiness through trial networks, centralized contracts, and centralized ethics processes, to ensure faster launch. • Enhance relationships among industry, government, and academia to optimize nimble research conduct. • Enhance governance structure (e.g., representation from provincial/territorial research funders and strategic research advisory committees) and create tighter linkages (e.g., through regular communication) between federal and provincial/territorial research funders. This will enhance communication and coordination, and will decrease duplication of efforts and potential research waste. • Ensure interdisciplinary engagement including those from non-health disciplines (e.g., social sciences, education, environment). |
Table 3.
| Topic | Participant responses |
|---|---|
| What participants did in this area | • Highlighted the importance of research into underlying conditions and chronic non-communicable diseases throughout the COVID-19 pandemic. • Facilitated continuity of funds (and extended timelines) for researchers who were unable to do their research because of COVID-19 restrictions. • Created extramural research networks (i.e., research that receives funding from sources other than universities) to enable scientific endeavour in particular areas (such as One Health). • Supported research that led to interdisciplinary research teams across the country. |
| What participants wish they had done differently in this area | • Develop better financing strategies for research. • Develop better salary support for researchers working in research institutions. • Pay more attention to supply chain issues in research. • Have a greater balance between COVID-19 research and non-COVID-19 research. • Create more funding opportunities for Indigenous researchers. • Avoid duplication of funding for research projects. |
Table 4.
| Topic | Participant responses |
|---|---|
| What participants did in this area | • Surveyed chief science officers and institutions about their research capacity and created a new funding program to invest in biocontainment laboratories in academic settings. • Targeted capacity building for early- to mid-career researchers. |
| What participants plan to do in the future in this area | • Recruit more researchers into government sectors. • Identify strategies to support the career progression of government scientists. • Facilitate rapid data sharing between provinces/territories, and support infrastructure to facilitate such communication and data sharing beyond COVID-19-related research. • Advocate for accessibility of national/provincial/territorial health data to facilitate research. |
| What participants wish they had done differently in this area | • Enhance infrastructure for therapeutics development. • Create linked, coordinated transdisciplinary networks in areas such as knowledge synthesis, vaccines, diagnostic testing, therapeutics, and implementation. |
Table 5.
| Topic | Participant responses |
|---|---|
| What participants did in this area | • Worked closely with partners, from co-production of research to dissemination of the results to decision-makers. • Used partnerships and a top-down approach to influence health service delivery through research. |
| What participants plan to do in the future in this area | • Change priorities to focus on COVID-19 recovery and broader (e.g., humanities, social science) long-term impacts of the pandemic. • Change the grant peer review process to reduce the delay between grant submission and funding decisions/distribution. • Connect with international institutions and partners with similar research agendas, to avoid duplication and enhance collaboration. |
| What participants wish they had done differently in this area | • More focus on coordinated evidence synthesis and dissemination, including to inform priority setting for research. • Fund large randomized trials that use innovative methods to allow for an evolving evidence base. • Link with international partners on randomized trials using pre-approved protocols. • Embed randomized, networked trials within the health care and public health systems. |
Knowledge exchange session 2
Leadership from research institutes attended session 2. Twenty-two individuals, representing 19 organizations, participated in this session. The 22 participants represented organizations in Canada (95%, n = 21) and New Zealand (5%, n = 1). All participants spoke English. Tables 6–9 summarize key themes related to what participants did, what they plan to do in the future, and what they wish they had done differently across each of the four functions of the WHO health research system framework (Pang et al. 2003).
Table 6.
| Topic | Participant responses |
|---|---|
| What participants did in this area | • Ensured that researchers and clinicians had access to biological samples for COVID-19 research. • Harmonized research ethics systems across regions. • Hired staff to focus on health equity in COVID-19 research. • Held events online rather than in person, to optimize accessibility. • Developed pan-Canadian networks to respond to research calls (e.g., Coronavirus Variants Rapid Response Network). • Centralized trial recruitment, to facilitate recruitment of participants across multiple COVID-19 trials. • Convened regular meetings of organizations’ research leaders to discuss activities that affected multiple institutions, such as funding and coordinating research. • Revisited research conduct and regulations, including development of standardized procedures for conducting trials in unconventional settings (e.g., patients’ homes). |
| What participants plan to do in the future in this area | • Continue to hold online/hybrid events, to maintain the accessibility of these events. |
| What participants wish they had done differently in this area | • Create a pan-Canadian data ecosystem to share data to improve the quality and speed of research. • Create a universally accessible biobank, to improve the quality and speed of research. • Centralize and accelerate processes such as ethics and contract approval across institutions and provinces/territories. • Have common electronic patient records across regions, and facilitate access to these data. • Have meaningful relationships with Indigenous leaders, to support their research needs. • Ensure that organizational staff members reflect the diversity of the population. • Facilitate pan-Canadian policy-maker support for clinician involvement in research. • Develop an emergency preparedness plan for research that includes plans for data sharing, cybersecurity, and infrastructure. • Implement a pan-Canadian research coordination infrastructure to support research activities, such as centralized patient recruitment for clinical trials embedded in the health and public health systems. • Work with funders from other countries to prioritize who will do what research according to each country’s specialties and capacities, to distribute priorities and avoid duplication of work. • Create a collaborative, nimble, responsive, pan-Canadian platform for conducting clinical trials. • Create a nimble system for synthesizing and disseminating/implementing clinical trial findings, which could support policy-makers’ and clinicians’ decision-making processes. • Use Canada’s provincial/territorial health and public health care systems to evaluate impact of different mandates/recommendations for COVID-19 management. |
Table 7.
| Topic | Participant responses |
|---|---|
| What participants did in this area | • Tracked and shared with policy-makers existing funding sources, which allowed organizations to advocate for support when COVID-19-related emergencies shut down external research funding, which in turn carried a risk of job loss. • Accessed unrestricted funds and resources so that research projects could be executed quickly. • Accelerated the grant peer review process. • Created a retention program to support salary for research personnel. • Developed pan-Canadian networks on specific research topics, to facilitate collaboration and coordination. • Partnered with federal government agencies to quickly disseminate funding information to these agencies. • Identified opportunities for researchers to collaborate on funding proposals. • Required all funded research to consider the health advancement of those marginalized by systemic injustice and to integrate equity into research funding plans. • Required all funded research to publicly disclose results immediately in line with other international funders to support rapid data sharing. • Streamlined format and timeline flexibility for researchers to complete research grant applications, achieve milestones, and report their findings. |
| What participants wish they had done differently in this area | • Provide more funding to support salaries for students, research staff, and researchers, to facilitate retention. • Establish health network research hubs to coordinate start-up research incubators and businesses. • Address how some research sometimes goes unfunded because it does not meet certain traditional standards of methodological excellence. • Increase funding for knowledge mobilization activities. • Provide more dedicated time and funds for clinician-scientists to do research, or build structures that allow them to do both clinical work and research. • Create a pan-Canadian data set on the collective impact of health research investment across all funders (e.g., federal-, provincial- and territorial-level funders and non-governmental organizations). • Fund larger, more coordinated clinical trials, instead of multiple smaller trials on the same topic, to facilitate research impact. • Optimize timelines for funding competitions, to ensure equitable access to each competition among researchers, while still responding to the urgent data needs of decision-makers. |
Table 8.
| Topic | Participant responses |
|---|---|
| What participants did in this area | • Created accommodations for trainee researchers (e.g., allowed Master’s and PhD students living in other countries to enroll virtually and maintained financial support for them). • Supported hospitals (where such support had not previously existed) to rapidly set up research, in particular clinical trials, and trained clinicians in research practices. • Advocated for infrastructure to support integration of research into practice and policy. • Ensured that research trainees and students were paid fairly. • Introduced additional leave days that could be taken anytime, without warning or explanation, in addition to sick days, to facilitate retention. • Implemented additional workplace supports such as flexible work hours. |
| What participants wish they had done differently in this area | • Support researchers without Canadian citizenship whose documentation had expired because of backlogged government systems and who consequently lost eligibility for grant funding. • Develop a plan for emergency preparedness, encompassing data sharing across Canada and cybersecurity (including considerations of remote access). • Create infrastructure (e.g., websites) and dissemination strategies to showcase what an organization, region, or country can offer in terms of research, with linkage to the health system. • Create more opportunities for researchers to commercialize their research or to efficiently start small or medium enterprises. • Use data and modelling to predict resource needs (e.g., workforce and equipment). • Use data to understand research workforce needs, including ensuring that research staff reflect the diversity of the population. • Use sustainable funding to invest in knowledge brokers (i.e., individuals who understand the evidence needs of health system leaders and can develop relationships to increase evidence uptake). • Facilitate patient access to clinical trial opportunities as part of treatment options in hospital-based trials, community-based trials, and decentralized trials, especially in rural, remote, and northern areas. |
Table 9.
| Topic | Participant responses |
|---|---|
| What participants did in this area | • Held science communication courses for knowledge users (e.g., policy-makers and members of the public). • Required plans for patient engagement and knowledge mobilization in grant applications. • Developed a knowledge mobilization, consultation, and support service for researchers, to increase patient engagement in the research process from the grant writing stage to knowledge dissemination. • Communicated the research through various media, such as opinion pieces for newspapers, podcasts, and webinars. • Hospital staff and researchers had regular conversations with decision-makers and government to facilitate knowledge mobilization of research findings. • Worked with patients to determine COVID-19-related research questions that the patients and their families cared about. • Co-developed knowledge mobilization materials with the target audience (e.g., children helped to develop videos and related materials on masking and vaccination directed toward other children). • Developed research briefs to disseminate research. • Monitored what non-COVID-19 research was paused or not funded, with a view to determining how to restart or begin the work. • Developed virtual knowledge mobilization activities. • Created roles for knowledge brokers to conduct rapid knowledge mobilization across several projects and to set up a knowledge mobilization network. • Included relationship-building requirements in research grants, to support knowledge mobilization of findings. • Developed a panel of early career researchers doing knowledge synthesis work, to share research, connect researchers to decision-makers, and provide researchers with exposure to the decision-making process. • Held events with researchers to discuss their challenges in building relationships with decision-makers. • Used researchers and patients’ personal impact stories to convey the value of health research to policy-makers and the public. • Developed the Pan-Canadian Health Data Strategy to support sharing of data across organizations. • Developed strategies to link researchers with policy-makers. |
| What participants wish they had done differently in this area | • Hold science communication courses and include both knowledge developers and users (e.g., traditional media, patient partners, and the public). • Address the fear of some researchers that they would forgo opportunities to publish if they share data with decision-makers before publication. • Use the pandemic as an opportunity to communicate what science is and what it is not, as well as how changing and evolving evidence can lead to inconsistent and evolving policy decisions. • Link science writers with researchers and patients to craft messages about research findings for the public, and have experienced communicators share these messages with the public. • Invite patient partners to be authors on academic papers. • Tailor knowledge mobilization events such as webinars to specific audiences. • Have a broader patient partner base, to decrease the burden on existing patient partners, and ensure they are fairly compensated. • In funding calls, include links to resources (e.g., people, services, or organizations) related to knowledge mobilization and patient engagement, to facilitate partnerships between researchers and knowledge mobilization services. • Collect and present data on the return on research investment for research users (e.g., decision-makers, patients, members of the public, and clinicians). • Provide time and support (e.g., graphic design, media training, financial support, and legal support) for researchers and clinicians to disseminate their research and to do media work or act as spokespeople for the research, especially when the content is controversial or abusive responses are anticipated. • Maintain strong relationships with patient partners. • Develop a pan-Canadian strategy for implementation science. • Link knowledge synthesis researchers to decision-makers. |
Knowledge exchange session 3
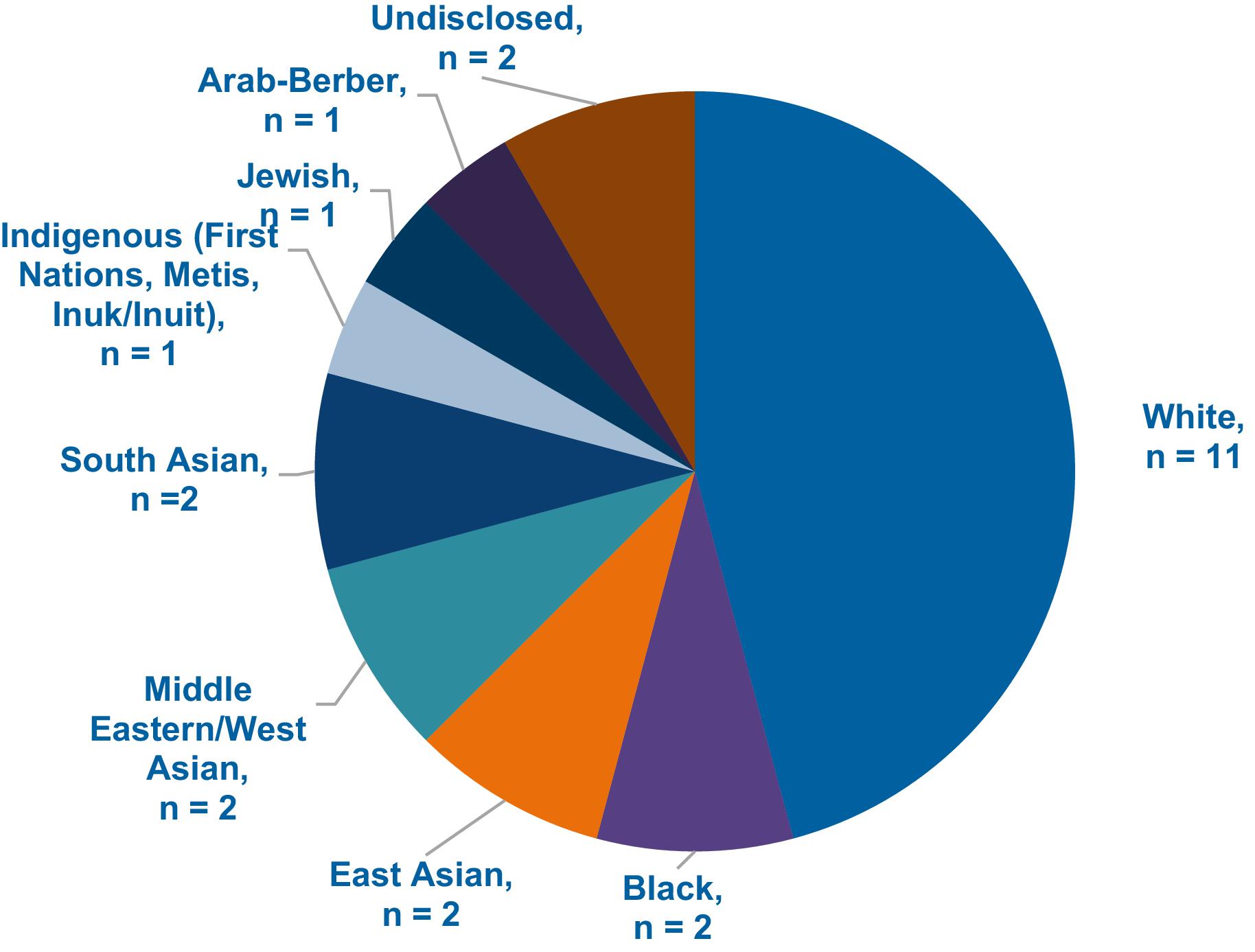
Members of the public and researchers attended session 3. Twenty-three individuals participated in session 3. Fifteen participants were members of the public and eight were researchers. All participants lived in Canada. Participants spoke both English (91%, n = 21) and French (9%, n = 2). Ten participants were women (43%), 10 participants were men (43%), two participants were non-binary (9%), and one participant did not disclose their gender. For the majority of participants, self-identified racial background was white (48%, n = 11), followed by Black (9%, n = 2), East Asian (9%, n = 2), Middle Eastern/West Asian (9%, n = 2), South Asian (9%, n = 2), Indigenous (First Nations, Metis, Inuk/Inuit) (4%, n = 1), Jewish (4%, n = 1), Arab-Berber (4%, n = 1), and undisclosed (9%, n = 2). Participants could select multiple racial background categories; therefore, the numbers do not sum to 23. See Fig. 1 below for racial and ethnic backgrounds of all participants.
Fig. 1.
Tables 10–13 summarize key themes related to what participants thought research funders, policy-makers, and researchers should do in the future across each of the four functions of the WHO health research system framework (Pang et al. 2003).
Table 10.
| Group | Participant responses |
|---|---|
| Research funders | • Redefine research excellence to include more than randomized controlled trials and journal publications (i.e., incentivize different ways to create and mobilize knowledge). • Increase collaboration between provincial/territorial ministries of health and national funding agencies like the CIHR, to develop collaborative research projects across ministries. Such projects should be developed with patient partners and should be considered through equity, diversity, inclusion, and anti-racism lenses. • Harmonize research ethics boards across institutions and provinces/territories. • When monitoring and evaluating research projects, include multiple parameters for success, particularly ones that entail asking the communities involved whether they were affected in any way. • Take more responsibility for ensuring that research is conducted ethically, for example, by offering ethics capacity building for researchers and acting as an arbiter for disputes between study participants and researchers. • Allow postdoctoral researchers to be principal investigators on funding applications or allow them to collaborate on applications to give the next generation of researchers relevant experience, including experience in developing programs of research at their institutions. • Specify patient engagement requirements in grant calls, and include requirements to ensure that the patient sample is diverse or representative of the research population. Include suggestions to allow for engagement between policy-makers and patient partners. • Develop a centralized list of health research priorities that includes input from patients/members of the public and policy-makers. Such a list of priorities could act as inspiration for researchers in their choice of topics. • Set up infrastructure to respond to emergency situations (including pandemics) to allow a rapid funding response. • Recognize the role of white supremacy and colonization in shaping health research systems (e.g., through its reward structure). Take steps to mitigate this, for example, by providing communities traditionally excluded from and harmed by research with more funding and autonomy to carry out research themselves, by ensuring more representation from these communities in decision-making positions, and by establishing less competitive grant models. • Increase salary/wages for researchers to keep up with the cost of living and to encourage careers in research. Specifically, funders could increase scholarships and stipends for trainees and postdoctoral researchers. • Require community engagement and relationship development from project onset, so that engagement is not tokenistic; include this goal in organizational mandates and priorities. • When developing priority areas for research or when developing research institutes/departments, have discussions with and recruit community members and those with relevant lived experience into research leadership roles. Gain insight from community members on what is the core problem and whether it is something that needs to be addressed. • Implement a system for peer reviewing the peer reviewers, to allow oversight of the peer review process and address systemic funding issues (e.g., systemic bias in funding decisions). |
| Policy-makers | • Update intellectual property policies to encourage work in areas that may not be financially lucrative. • Develop better data-sharing systems and systems of health research collaboration among provincial/territorial ministries in Canada. • Encourage more researchers to enter public health policy, with a view to reducing the political influence on science. • Create an international consultative panel independent of government, to provide recommendations based on health research in times of crisis. • Where possible, include patients as equal partners at the governance decision-making levels. • Facilitate representation of all provinces and territories at decision-making levels to support coordination. • Fund research on how the health care system is operating, to determine how it can better serve the public. • Develop a list of priorities across provinces and territories and determine which locations/research programs are best suited to conduct research in each priority area. • Research funding agencies and government ministries of health are working separately to create engagement opportunities between patient partners and policy-makers; they should increase their collaboration in this area. • To prevent researchers and research staff experiencing marginalization from being pushed out of the workplace, put in place strong policies to investigate, address, and monitor complaints about discrimination or microaggressions. • Develop an independent body of policy-makers to weigh research requirements among COVID-19 research, non-COVID-19 research, and capacity building, and determine how funding should be balanced among these three areas. |
| Researchers | • Evaluate the research experiences of patient partners throughout the COVID-19 pandemic. • Aim for research teams that are reflective of the relevant research population, with lived experience in the topics that are being researched. |
Note: CIHR, Canadian Institutes of Health Research.
Table 11.
| Group | Participant responses |
|---|---|
| Research funders | • Include patients and people with lived and living experience on panels for review of research funding calls. • Create or incentivize collaborative rather than competitive grants. To do so, reconsider the common “grant model” for financial support and instead consider models in which researchers are not responsible for bringing funding to their university or hospital. • Consider programmatic funding, as opposed to, or in addition to, project funding. Such funding involves base support, with additional funding for specific research projects. • Encourage research collaboration and joint research funding models across countries and create legal, IP, and data sharing agreements. • Increase flexibility in research project timelines, to ensure that patient engagement and knowledge mobilization activities are conducted with care, while balancing the need for timely responses to urgent research calls during emergencies. This balance could be facilitated through establishing relationships and networks pre-emergency. • Ensure that research priorities and funding allocations are transparent. • Track and publicize which research proposals are funded and which are not funded, to help researchers understand which research questions are more likely to receive funding. • Implement systems at research institutions and funding agencies to allow appropriate funding for patient partners. • Ensure that funding calls include requirements for the research team to have identities similar to those of the research population. • Ensure that funding calls include requirements for diversity among patient partners. • Consider equity, diversity, inclusion, and anti-racism at each step in the research project, including in grant applications. • Balance research on COVID-19, “long COVID”, and other diseases/conditions. • Invest in research into the indirect impacts of COVID-19 (e.g., on education, on mental health, and on health care providers). • Given that health care providers are paid significantly more for clinical work than for research work, provide salary support for clinician researchers, to encourage research and demonstrate its importance. • During emergencies, reduce the intensity of grant requirements, given the amount of time and resources required to prepare grant applications and given that many applications are unsuccessful. • Reduce the competitiveness of funding by reducing application requirements and developing more collaborative grants. • Ensure that a portion of grants is reserved for early career researchers. • Ensure that funding allocation decisions throughout each research competition are transparent. • Reduce the fees for journals’ open-access publication, and impose limits on those fees. |
| Policy-makers | • Although there are ethical issues with seeking research funding from private funders (e.g., conflicts of interest and influence on research priorities), ethical issues also arise when research funding for critical health issues is lacking. Weigh these ethical issues to help decide where research funding should be sought. • Encourage standardization of participant compensation across the country. • Adjust rules related to patents and intellectual property for vaccines and other therapeutics, to allow for greater distribution of these research products. • Encourage collaboration among industry partners (e.g., pharmaceutical companies) in the development of therapeutics, diagnostics, vaccines etc., to increase effectiveness and the speed of development and to reduce the funding required. • Encourage industry partners (e.g., pharmaceutical companies) to cycle the profits made from COVID-19-related products and services back into the health research system to fund additional health research. • To increase available research funding, require higher-income individuals and corporations (especially those who profit from population health issues, such as pharmaceutical companies) to pay more taxes. • Take responsibility for the funding cuts made before the pandemic that had harmful effects on the health care and health research systems. Take steps to re-invest in health care and health research. • Increase remote work and work-from-home opportunities for researchers, to increase collaboration across various communities, to bring new perspectives to research questions, and to potentially reduce the cost of some research activities. • Encourage private research funding options, so that researchers have more options when applying for continuation of funds. |
| Researchers | • Set up systems for crowd funding of research projects, and ensure that this is done ethically. • Conduct research into public uptake/understanding of science and how this can be improved. • Conduct research on the reasons for migration of health care workers across provinces/territories and why health care workers are lacking in some regions. |
Note: IP, intellectual property.
Table 12.
| Group | Participant responses |
|---|---|
| Research funders | • Expand the pool of patient partners involved in grant peer review. • Ensure that researchers and research staff across experience levels are paid an attractive wage that allows them to support themselves and their families. Support job security for researchers and research staff. |
| Policy-makers | • Reduce barriers (e.g., financial and lack of representation) that prevent populations less commonly represented in research and policy-making from entering these fields. Ensure they are aware of the range of research-related positions, including principal investigator, biostatistician, laboratory technician, research coordinator, knowledge broker, and policy-maker. • Invest in engaging young people (e.g., high school age and undergraduates) in research by introducing them to research concepts, fields, and careers through programs such as boot camps and career days, and by providing guidance counsellors with relevant information. • Build capacity among policy-makers to understand and use evidence in decision making. |
| Researchers | • Ensure that research teams reflect the identities of their respective research populations, to provide insight on appropriate research questions, methods, inclusion criteria, etc. • Train researchers in the engagement of policy-makers. • Ensure that patient engagement methods have a trauma-informed lens and that engagement activities are safe spaces for individuals to contribute. Conduct training in these areas if needed. • Engage in training or other forms of capacity building to unpack and dismantle individual internal biases or discriminatory beliefs (e.g., racism, sexism, and ableism). |
Table 13.
| Group | Participant responses |
|---|---|
| Research funders | a. Require researchers to provide accessible, lay-language summaries of their research through written materials (e.g., infographics), on social media, or through events (e.g., CIHR’s Café Scientifique). b. Develop communication plans to convey to the public the importance of health research in general and why the public should care about and engage in research. c. Include requirements for meaningful and transparent patient engagement as part of the ethical standards for research projects. d. Consider funding social media or marketing positions in research laboratories and research programs. Consider hiring university students interested in both research and communications for these positions. e. Create educational courses or seminars on research directed toward patient partners, to increase patients’ understanding of their role on a research team and to increase their engagement. f. Develop and fund a pan-Canadian database that allows patients and researchers to connect for patient engagement or project recruitment purposes. g. Allow patient partners to use abbreviated Common CVs when applying to participate in research. Ensure that they are not asked to supply personal information (e.g., home address). |
| Policy-makers | • When instituting change in public health practices, invite community leaders (e.g., religious leaders) to attend information sessions where they can ask questions, voice concerns, and build relationships with the policy-makers, with a view to having them disseminate this information to their community members. • Increase public transparency related to investments in and outcomes of health research. • Increase accountability and transparency for determining whether and how policy-makers follow research evidence and apply the evidence to their decision-making. Evaluate whether and how policy-makers’ decisions are informed by evidence. • Develop a centralized list of research opportunities for patient partners by institution and province/territory. • Invest in marketing and promotion of health research in Canada, as well as in removing misinformation. Use a range of approaches (with consideration of the population targeted by the research), such as social media, community leaders, and community organizations (e.g., faith organizations, information centres, and youth centres). Use community connections to disseminate this information, to increase trust. • Consider how to build a future of health care research where every encounter with the health system is an opportunity for research/evaluation. • Build knowledge mobilization capacity among policy-makers. |
| Researchers | • Increase accessibility of research to research participants by offering the opportunity for researchers to travel to participants to collect data (as opposed to participants travelling to the researchers), offering evening and weekend options to participate, and providing various language options. Consider using community leaders (e.g., clergy) to support recruitment and data collection. Such efforts could promote diversity in the participant sample, given that the population available to participate in English during daytime hours is typically of higher income, retired, and white. • Increase involvement in health advocacy beyond the researcher’s own research projects. • Treat patient partners as research partners (e.g., include them as authors on manuscripts, ensure they have access to published articles, and engage them in knowledge mobilization activities). Consider giving patient partners concrete roles within the research project. • Invest more time in marketing and promotion of research participation and engagement opportunities to patient/community partners. Promote these opportunities on websites and social media platforms and through posters in community centres, parks, colleges, universities, and other locations where people gather. • When recruiting patients and community members for partnership or participant roles, recognize that some communities have a valid distrust of health care and health research systems due to historic and ongoing harm against certain groups (e.g., racialized and transgender populations). Acknowledge this issue during recruitment efforts, and aim to build collaborative, trusting relationships. • To increase transparency and dissemination, promote research projects to the research community, the public, and policy-makers while they are still in progress, providing updates on preliminary results. Avoid waiting until the end of the project to disseminate results. • Develop living systematic reviews that are accessible to the research community, the public, and policy-makers for specific health topics (e.g., COVID-19), to allow these audiences to stay informed about new evidence. • Budget for patient engagement throughout the project. • Consider engaging patients, particularly those with relevant lived experience, in fundamental or pre-clinical research. These perspectives can help shape the research question. • Incorporate patient partners across research activities, including formulating the question, developing methods, performing data analysis and interpretation, and conducting knowledge mobilization activities. • Evaluate the impact of knowledge mobilization on community health outcomes. • Provide research mentorship for patient partners. • Develop knowledge mobilization materials to communicate research that is transparent and accessible to the public, traditional and social media, and policy-makers. |
Note: CIHR, Canadian Institutes of Health Research; CV, curriculum vitae.
Survey 2
A total of 85 individuals completed survey 2. Just under half of the participants were from research organizations (49%, n = 42). Another third (32%, n = 27) were research users (e.g., members of the public or patients, government employees, journal staff, and health care providers), and smaller proportions were from health research funding agencies (2%, n = 2) and other types of organizations (e.g., health authorities and consultants) (16%, n = 14).
When asked which recommendations were of greatest importance for implementation in Canada, participants gave the highest ratings to recommendations that focused on prioritizing equity and anti-racism in research processes, improving patient engagement in research, enhancing emergency preparedness, increasing researcher and research trainee wages and development opportunities, and aligning and coordinating research priorities across different entities.
Common feedback from participants on the draft recommendations included a preference to avoid additional layers of oversight or bureaucracy across the research process, enthusiasm for harmonized research processes (e.g., research ethics board (REB) processes), and a desire to increase coordination among existing organizations.
Survey 3
A total of 54 individuals completed survey 3. Over half of the participants were from research organizations (63%, n = 32). About one quarter (24%, n = 12) were research users (e.g., members of the public or patients, government employees, journal staff, and health care providers), and smaller proportions were from health research funding agencies (6%, n = 3), government (2%, n = 1), and other types of organizations (e.g., advocacy organizations) (12%, n = 6).
Participants were asked to select their priority action for each recommendation. In the following section, actions are listed with the top two ranked appearing first and second and whom they felt should be responsible for their implementation.
Recommendations
From the results of the knowledge exchange sessions and surveys, the project team developed the following 12 recommendations to strengthen Canada’s health research system after the COVID-19 pandemic. The recommendations are organized according to the four functions of the WHO health research system framework (Pang et al. 2003). From the results of the sessions and surveys, we also developed potential actions to accompany each recommendation to support the implementation of the recommendations. Each of these actions will require careful consideration by interested parties across jurisdictions to consider implementation feasibility and to prioritize.
Function 1: governance/stewardship
Recommendation 1: outline research logistics as part of emergency preparedness to streamline research in future pandemics
a.
Develop an emergency preparedness research plan that encompasses data sharing (across provinces/territories and federal partners), cybersecurity, REB approvals, protocols for key studies on health emergencies that have been pre-cleared by an REB, supply chain procedures, and a One Health (https://www.who.int/news-room/questions-and-answers/item/one-health) approach.1
b.
Harmonize processes (relating to aspects such as data collection, privacy, and database searchability) for biobanks (repositories of biological samples that are used in research) and data sharing (the dissemination and exchange of data/research findings for the purpose of further research) within and across provinces/territories, to facilitate rapid initiation and performance of research.*
c.
Develop an emergency preparedness research plan that coordinates research questions for prioritization by international research funders based on capacity, expertise, and infrastructure, and ensure that the plan is fully integrated with existing research policies.
d.
Centralize, standardize, and harmonize REB processes nationally, by using a single online application form and centralized intake process, with reviews distributed to regional REBs according to their wait times, standardized training, and tracking of timelines.
e.
During health/public health emergencies, prioritize REB review for relevant studies, maintaining an equity focus in the research.
Who should be responsible for implementing the actions (according to survey respondents): Overall, respondents felt that all actors in the health research ecosystem should be responsible for these actions including the CIHR, Public Health Agency of Canada (PHAC), Health Canada, provincial and territorial governments, universities, research institutes, and provincial and territorial funding agencies.
1
Participants were asked to select their priority action for each recommendation. Actions are listed with the top two ranked appearing first and second.
Recommendation 2: embed equity and inclusion in all research processes
a.
Use equity and anti-oppression principles in all governance decision-making and activities and ensure alignment with the Tri-Council Agencies’ Dimensions Charter (https://www.nserc-crsng.gc.ca/InterAgency-Interorganismes/EDI-EDI/Dimensions_Dimensions_eng.asp) and the rights of First Nations, Inuit, and Métis peoples (e.g., United Nations Declaration On The Rights Of Indigenous Peoples (https://social.desa.un.org/issues/indigenous-peoples/united-nations-declaration-on-the-rights-of-indigenous-people)).*
b.
Include patients/members of the public at all governance levels in the health research ecosystem, using an open and transparent recruitment process, and publicly report on their inclusion.*
c.
Create a pan-Canadian database of ongoing studies with which patients can engage as both research partners and research leads.
Who should be responsible for implementing the actions (according to survey respondents): Overall, respondents felt that the CIHR, provincial and territorial governments, research institutes, and provincial and territorial funding agencies should be responsible for these actions.
Recommendation 3: facilitate streamlined, inclusive, and rigorous processes for grant application preparation (e.g., by research institutes) and review (e.g., by funders)
a.
Ensure that equity and diversity principles are embedded within all requests for proposals and grant applications, including the consideration that the research team and patient partners should reflect the diversity of the relevant population and that study team and participant demographic characteristics are reported to granting agencies to ensure they are reflective of the study population.*
b.
Monitor grant application and success rates through applicants’ PROGRESS PLUS (https://methods.cochrane.org/equity/projects/evidence-equity/progress-plus) factors (an acronym used to identify characteristics that stratify health opportunities and outcomes) and sex- and gender-based analysis plus (GBA± (https://www.womensacademics.ca/sex-gender-based-analysis-plus/)), report on this information publicly, and use it to inform and revise grant competitions (e.g., to prioritize specific research areas or researchers who are experiencing structural barriers).*
c.
Reimburse peer reviewers for any caregiving support required for their dependents, to enable the peer reviewers to attend meetings (e.g., as implemented at the CIHR (https://cihr-irsc.gc.ca/e/51947.html)).
d.
Ensure that peer reviewers are trained in anti-oppression in research, as well as in equity, diversity, and inclusion principles.
e.
Mandate that principal investigators with peer-reviewed grants must participate in grant peer review for the duration of their grant support.
f.
Ensure flexible virtual and hybrid processes for grant peer review.
g.
Include patients in grant peer review processes.
h.
Ensure that patient peer reviewers are adequately compensated, to ensure they have capacity to participate as peer reviewers.
i.
When reviewing grants, use PHAC’s strengthening the Integration of Intersectionality Theory in Health Inequality Analysis checklist (https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/science-research-data/how-integrate-intersectionality-theory-quantitative-health-equity-analysis/phac-siithia-checklist.pdf) to assess whether and how research applicants adhere to equity considerations.
j.
Create transdisciplinary (e.g., reflective of the CIHR's 4 pillars of health research (https://cihr-irsc.gc.ca/e/37788.html)) grant peer review panels, and provide peer review training for transdisciplinary research.
k.
Create iterative grant peer review processes, with opportunity for interviews with applicants and the peer review panel to clarify questions/responses.
l.
Streamline the grant application process for patients, through methods such as reducing requirements for patients to complete letters of support, CVs, and GBA± (https://www.womensacademics.ca/sex-gender-based-analysis-plus/) modules and including patient-friendly instructions and modules.
m.
Conduct peer review of the grant peer review process (including review of the peer reviewers), and make the results of this peer review transparent.
n.
Where possible, provide flexibility in deadlines for applications (e.g., frontline workers).
o.
Provide networking opportunities for shortlisted or higher ranked applications.
Who should be responsible for implementing the actions (according to survey respondents): Overall, respondents felt that the CIHR, provincial and territorial funding agencies, and research institutes should be responsible for these actions.
Recommendation 4: create knowledge mobilization infrastructure to support the generation and use of evidence
a.
Develop centralized processes to communicate and coordinate research priorities with knowledge users (e.g., researchers, academic institutions, charitable organizations, and patient/public organizations, including equity-deserving groups). Share communications in several languages to reflect languages spoken by people in Canada.*
b.
Develop protocols and processes for rapid funding calls (e.g., ensuring they include a focus on populations that may be at highest risk of health inequities).*
c.
Encourage the use of communication platforms across the funders including Tri-Council Agencies and international funding agencies, to facilitate alignment of research priorities in pandemics/health emergencies and to coordinate research-related communication (e.g., Global Research Collaboration for Infectious Disease Preparedness (GloPID-R))(https://www.glopid-r.org/).
d.
Develop principles of transparent communication related to what research is funded, including publicly reporting data on research impact and the overall impact of research funding to take the opportunity to build on the enhanced recognition of the benefits from health research that developed during the pandemic.
Who should be responsible for implementing the actions (according to survey respondents): Respondents felt that the CIHR, PHAC, and Health Canada were largely responsible for these actions.
Recommendation 5: coordinate research efforts across local, provincial, national, and international entities
a.
Leverage and extend use of the Canada Research Coordinating Committee (CRCC)(https://www.canada.ca/en/research-coordinating-committee.html) to provide research and innovation advice, oversight, democratic decision-making, coordination, prioritization, and communication across the Tri-Council Agencies (https://research.utoronto.ca/engaging-research/tri-agency-policies-guidelines-initiatives) and the Canada Foundation for Innovation (CFI)(https://www.innovation.ca/) and among international funding agencies.*
•
Membership in the CRCC should be broad and include national (e.g., CIHR (https://cihr-irsc.gc.ca/e/193.html), Health Canada (https://www.canada.ca/en/health-canada.html), and PHAC (https://www.canada.ca/en/public-health.html)) and provincial/territorial (e.g., National Alliance of Provincial Health Research Organizations (NAPHRO)) (https://www.naphro.ca/) funding agencies.
•
This wider use of the CRCC could be achieved, for example, through strategies to create better coordination, as suggested in the recent report of the Advisory Panel on the Federal Research Support System (Government of Canada 2023).
b.
Establish a health research funding entity in each province/territory where these do not currently exist, through which the provincial/territorial health ministry and public health agency can connect on research priorities and evidence needs.*
Who should be responsible for implementing the actions (according to survey respondents): Respondents felt that Health Canada, the CIHR, and provincial and territorial funding agencies and governments should be responsible for these actions.
Function 2: financing
Recommendation 6: reimagine the funding of health research
a.
Ensure long-term funding for successful research enterprises, and develop strategies that balance defunding of low-impact initiatives with funding for exploratory research.*
b.
Establish funding and sustainability strategies for provincial/territorial health research hubs, with linkages to health, public health, social care, education, animal and environmental health, and cross-disciplinary collaborations.*
c.
Embed equity considerations into decision-making for all research investments, such as making funding contingent on meaningful actions to address inequities.
d.
Assess the extent to which research infrastructure and associated funding exist for therapeutics, vaccines, and the development and implementation of diagnostic tests, and develop metrics for appropriate allocation.
e.
Increase overhead/indirect cost allowances (i.e., costs of doing research, including costs for space, human resources, and contract support) for research institutes (e.g., to 50%) to cover the cost of research operations.
f.
Engage with industry to facilitate transparent contributions to funding and transparent communications with health research authorities/hubs/networks/platforms.
g.
Work with industry to generate unrestricted funds for project research grants and infrastructure grants, with transparency protocols.
h.
Ensure separate funding for research driven by knowledge users and research driven by researchers.
i.
Support mechanisms for crowdfunding research.
j.
Provide more support for researcher success (e.g., increase funding pool and/or support increased quality of applications).
k.
Increase access to research funding pools for non-academic organizations (e.g., local health authorities).
l.
Specify funding requirements and fund access to support involvement of patients as research partners (e.g., through honoraria, translation, and child care), while considering patients’ financial circumstances (e.g., implications for disability-related income, tax implications).
Who should be responsible for implementing the actions (according to survey respondents): Respondents felt that the CIHR, provincial and territorial governments, and funding agencies should be responsible for these actions.
Function 3: capacity building
Recommendation 7: invest in formative training opportunities rooted in equity, diversity, and anti-racism
a.
Embed formative equity, diversity, inclusion, and anti-racism components in all research capacity-building activities.*
b.
Provide collaborative training for researchers, patients, and policy-makers on patient engagement and knowledge mobilization.*
c.
Provide training for researchers on trauma-informed approaches to patient engagement, that is, approaches rooted in an understanding of how trauma affects people, with the purpose of avoiding potential re-traumatization during the research process. These approaches would also acknowledge broader social contexts and how systems of oppression (e.g., colonialism and white supremacy) cause trauma.
d.
Provide training for researchers, patient partners, and policy-makers on anti-oppression practices in research, that is, practices that name and seek to dismantle injustices and power imbalances in the broader social context and in the specific research processes (e.g., asking community members most affected by the research to lead key research activities, such as developing the project plan and the budget). Integrate inclusive writing training for researchers and policy-makers (e.g., anti-racist language).
e.
Establish a transdisciplinary, pan-Canadian standard for engaging patients as partners in research.
f.
Increase opportunities for the full range of clinical staff to build their research capacity.
Who should be responsible for implementing the actions (according to survey respondents): Respondents felt that the CIHR, universities, research institutes, and provincial and territorial funding agencies should be largely responsible for these actions.
Recommendation 8: support researchers’ career development throughout their career span
a.
Use provincial/territorial/national data and dynamic modelling to estimate needs for the health care workforce and the research workforce (e.g., align training opportunities while monitoring for burnout/lack of retention).*
b.
Create salary support pathways for scientists and clinician-scientists (such as salary support awards or embedding of salary into grants) throughout their career trajectories, from early- through mid- to senior-career phases.*
c.
Create pan-Canadian support strategies for those disproportionately affected, both systemically and during the pandemic, such as Black, Indigenous, and people of colour (BIPOC), women, and non-binary people. Clinician-scientists were also disproportionately affected during the pandemic because of increased clinical work.
d.
Provide sufficient funding for researchers to engage in knowledge mobilization, including funding for communications, media, and graphic design.
Who should be responsible for implementing the actions (according to survey respondents): Respondents felt that provincial/territorial funding agencies, the CIHR, and research institutes should be responsible for these actions.
Recommendation 9: support early career researchers to establish themselves
a.
Create transdisciplinary research training networks for graduate students, fellows, and early career researchers, to facilitate research and research training in diverse methods and disciplines (e.g., implementation science, One Health (https://www.who.int/health-topics/one-health#tab=tab_1), and artificial intelligence) across all of the CIHR health research pillars.*
b.
Create opportunities for post-doctoral fellows to work in more than one sector (academic, industry, or government) during a fellowship.*
c.
Create pathway to independence awards to support early career researchers to transition from mentored research roles to independent research careers.
Who should be responsible for implementing the actions (according to survey respondents): Respondents felt that universities, the CIHR, research institutes, and provincial/territorial fund agencies should be responsible for these actions.
Function 4: producing and using research
Recommendation 10: strengthen Indigenous health research and break down systemic barriers to its conduct
a.
Incorporate guidance and knowledge to support respectful research engagement with Indigenous people, including the OCAP principles (https://fnigc.ca/ocap-training/)(ownership, control, access, and possession), the OCAS principles (https://umanitoba.ca/health-sciences/sites/health-sciences/files/2021-01/framework-research-report-fnmip.pdf) (ownership, control, access, and stewardship), and Inuit Qaujimajatuqangit (https://www.nccih.ca/en/publicationsview.aspx?sortcode=2.8.10.16&id=6) (Inuit traditional knowledge).*
b.
Remove barriers that prevent Indigenous knowledge keepers from being principal applicants for research funding.*
c.
Sustain Indigenous-led biobanks and data sharing.
Who should be responsible for implementing the actions: These actions should be led by Indigenous researchers and groups. To complement this, survey respondents felt that the CIHR, Health Canada, and universities should be responsible for these actions.
Recommendation 11: develop mechanisms to produce novel research
a.
Further develop collaborative transdisciplinary grants across the Tri-Council Agencies (leveraging the New Frontiers in Research Fund (https://www.sshrc-crsh.gc.ca/funding-financement/nfrf-fnfr/index-eng.aspx)) to support collaborations across research disciplines, for activities ranging from development of the team and the research project to completion and dissemination of the research.*
b.
Create partnership grants between researchers and knowledge users that focus on research uptake. Engage colleges for research and as knowledge users.*
c.
Create provincial/territorial health research hubs to link the health care delivery context with research across all of the CIHR health research pillars (https://cihr-irsc.gc.ca/e/37788.html). Include patient/public engagement and commercialization, and facilitate a pan-Canadian network of these hubs.
d.
Embed one or more clinical trial platforms within each health care delivery/health research hub.
e.
Engage patients/members of the public in prioritizing funding calls for research areas.
f.
Increase grant budgets for pilot studies/idea grants.
Who should be responsible for implementing the actions (according to survey respondents): Respondents felt that the CIHR, Health Canada, provincial and territorial funding agencies, and government should be responsible for implementation.
Recommendation 12: enhance research use across the health research ecosystem
a.
Create a network of chief science advisors in all federal/provincial/territorial government departments.*
•
Create opportunities for these advisors through knowledge exchange with researchers across Canada.
•
Enable these advisors to interpret and communicate science to policy-makers, including through communication of evidence uncertainty.
b.
Create knowledge exchange opportunities across funded networks/platforms/hubs.*
c.
Enhance science-to-policy dissemination training for researchers (e.g., training in plain language communication) and policy-makers through various approaches, including modules and embedded training opportunities.
d.
Co-create and deliver public education strategies for increasing health research literacy among members of the public.
e.
Co-create and deliver training for patients on engaging in research.
f.
Co-create and deliver training for patients on interacting with policy-makers.
g.
Improve provincial/territorial/national data banks (e.g., StatCan, Canadian Institute for Health Information, and granting agencies).
h.
Enhance research use through ensuring potential users are fully involved in priority setting and co-producing research wherever possible.
i.
Increase incentives for researchers to engage in activities to promote research use by emphasizing and embedding processes for research impact assessment.
Who should be responsible for implementing the actions (according to survey respondents): Respondents felt that all parties should be responsible for implementation including universities, research institutes, governments, and funding agencies.
Discussion
Threats to the health research system
The COVID-19 pandemic rapidly produced substantial changes in research conduct and in how research funders and researchers function including their engagement with policy-makers and other knowledge users. Participants in this project outlined some of the challenges faced in the research system in Canada during the pandemic and what strategies people implemented to try to mitigate them. While in some research areas the pandemic accelerated collaboration and innovation, in other areas it stalled or otherwise negatively affected research activities (Audisio et al. 2022). Globally, the pandemic yielded unprecedented collaboration across governments, research funders, and researchers such as initiatives focused on vaccine development and studies to understand seroprevalence of SARS-CoV-2 and immune correlates of infection (G20 Research Group 2020; Cai et al. 2021; Druedahl et al. 2021; Fanning et al. 2021; Kowalski 2021). Researchers developed new collaborations across different sectors such as with industry to support development of new diagnostic tests and treatments, geography and engineering to inform wastewater surveillance for SARS-CoV-2, and mathematical modellers and immunology researchers to develop and target new testing approaches (The COVID-19 Immunity Task Force 2021). Worldwide, the massive and rapidly evolving information demands of governments and the public created urgent needs for transparent evidence-based decision-making and evidence communication to ensure clarity and consistency of messages. These needs led researchers to develop partnerships with policy-makers at all government levels, health care leaders, and public health officials among others; it also underscored the need to consider the intersection between health, public health, social care, and education among other sectors.
The pandemic similarly exposed and exacerbated weaknesses in the health research system. Worldwide systemic bias and health inequities were exacerbated during the pandemic, making inequities for key groups not engaged in research (such as Black and Indigenous communities) worse (Khazanchi et al. 2020). These inequities highlighted the need for transformative action to address systemic racism within research, health care systems, and society.
The accelerated rate of production and volume of research during the pandemic supported the growth of preprint registries as repositories for research that has not been peer reviewed (Bauchner et al. 2020; Palayew et al. 2020; Caulfield et al. 2021); however, in many cases, this research was not published subsequently in a peer-reviewed journal, thereby threatening knowledge users’ trust in results. Alongside, there was substantial spread of myths and misinformation (Fahim et al. 2023; Theivendrampillai et al. 2023), which affects public trust in decision-makers and underscores the need for efforts to build public trust in science and government (Saitz and Schwitzer 2020; Caulfield et al. 2021).
Similarly, the pandemic produced disruption and yielded inequities across research institutions and researchers. For example, for long periods, basic science researchers were unable to access their labs placing their work, careers, and careers of their lab staff in jeopardy. In addition, health charities faced substantial reductions in financial donations, thereby decreasing research funding (Imagine Canada 2021; Breathe the Lung Association n.d.). These decreases in resources from health charities further stressed the already underfunded research pipeline, with the most notable impacts on trainees, early career researchers, and researchers from under-represented groups (including women, BIPOC, and disabled scientists). For example, studies showed that the gender gap in authorship of publications posted on pre-preprint registries grew significantly during the pandemic and women submitted fewer grant applications during this period with the results being worst for BIPOC women (Andersen et al. 2020; Myers et al. 2020; Narayana et al. 2020; Halley et al. 2021; Rabinowitz and Rabinowitz 2021; Staniscuaski et al. 2021; Mishra et al. 2023). Moreover, the impact on women researchers who are often the primary caregivers for children or older family members was dramatically impacted during the pandemic (Andersen et al. 2020; Halley et al. 2021; Staniscuaski et al. 2021; Davis et al. 2022). Studies also showed that women were more likely to take on COVID-related clinical and administrative work than their men counterparts were. As such, women physician scientists, in particular, those at early career stages face substantial challenges in recovering from the pandemic (Andersen et al. 2020; Myers et al. 2020; Narayana et al. 2020; Halley et al. 2021; Rabinowitz and Rabinowitz 2021; Staniscuaski et al. 2021). Similarly, for researchers able to pivot into COVID-19 research, the pandemic provided new opportunities, while those who could not pivot their research face a difficult and likely prolonged recovery period.
Actionable recommendations to meet these challenges
While some of these challenges within the Canadian health research system are longstanding, others represent new challenges that the pandemic has revealed; yet, all of these issues must be addressed to build robust health research systems. Various organizations and coalitions are beginning to address aspects of health research system recovery post-pandemic. However, increased coordination across initiatives, development of new initiatives, and purposeful action are urgently needed to develop an approach to facilitate pandemic recovery and transform the health research system to be more nimble, innovative, diverse, inclusive, equitable, and resilient.
We undertook an international initiative to identify potential solutions to these challenges. It included a series of knowledge exchange sessions and surveys to develop actionable recommendations to strengthen Canada’s health research system after the COVID 19 pandemic, to strengthen our health care and public health system, and embed health in all policy. Participants discussed how the pandemic response of Canada’s health research system could be strengthened through a variety of means, such as developing robust emergency and communications processes; prioritizing equity, diversity, and anti-racism; increasing coordination; revising funding processes’ investing in researchers, patient engagement, and capacity building; breaking down barriers to Indigenous-led health research; and producing innovative and useful research. Informed by the session and survey results, we presented 12 actionable recommendations that a range of organizations individually and in partnership can take to strengthen Canada’s health research system after the pandemic, some of which are in process.
Related work and placing this report in context
Our work is complementary to other initiatives that were conducted across different jurisdictions. Some provinces are examining their research response to the pandemic (e.g., British Columbia) and exploring what might be put in place to strengthen their health research systems (Michael Smith Health Research BC 2022; Michael Smith Health Research BC 2023). The CIHR, NAPHRO, and the Health Charities Coalition of Canada undertook discussions on the impacts, gaps, and opportunities in the Canadian health research landscape because of COVID-19 to identify areas for collective action among Canadian health research funders. In March 2023, the Advisory Panel on the Federal Research Support System (Government of Canada 2023) was released, following consultations with interested parties including researchers. It recommended to increase research funding, create a national research vision, and support coordination across research funders, among other suggestions. This Advisory Panel Report aligned with similar recommendations made in the 2017 Fundamental Science Review (Government of Canada 2017). There is a review underway of the federal approach to pandemic science advice and research coordination, which is expected to release recommendations in 2024. It will provide federal-level recommendations for future pandemics and other health emergencies on optimizing science advice impact, evidence synthesis coordination, and supporting efficient decision-making, including on research investments. Internationally, some countries are conducting reviews of their pandemic response, including that in research (UK Research and Innovation 2023; UK Covid-19 Inquiry 2024). And the journal Health Research Policy and Systems dedicated a theme issue (Health Research Policy and Systems 2021) to the role of health research systems in the control and management of COVID-19, so that the experiences of countries and their lessons learned could be shared.
There are common themes found across all of these reports including the need to increase research investment and enhance coordination. Similarly, recommendations are aligned on enhancing relationships between researchers and policy-makers and in supporting the development of research talent pathways. In particular, there is worldwide recognition of the importance of supporting graduate students, fellows, and early career researchers—who represent the future of science and innovation. Moreover, critical attention must be paid to anti-oppression and equity in research to address health disparities.
There are some different recommendations identified in this current report, which may be due to engagement of additional interested parties beyond researchers and policy-makers—namely members of the public. As such, there was a major theme and actionable recommendations on public engagement, which is critical to rebuild trust in science. Moreover, there was a theme and recommendations on enhancing capacity and methods for knowledge mobilization (including the science and practice of implementation) to optimize research uptake and a theme on breaking down barriers to Indigenous-led research.
Not all of the recommendations made in this current report will be immediately implementable and they will need to be prioritized, considering feasibility across jurisdictions. Moreover, their implementation must be contextualized in the current reality of health research funding in Canada. For example, the CIHR budget was $1.02B in 2014 and $1.2B in 2023 (HealthCareCAN 2023). Canada’s investment in research lags behind those of other Organisation for Economic Co-operation and Development countries. In 2022, Canada spent 1.5% of its gross domestic product (GDP) on research and development in comparison to 3.3% by Australia and 4.7% by the United States. Indeed, Canada is the only G7 country where research and development as a percentage of GDP has decreased over the past 20 years (OECD 2024).
There are several limitations to this project. First, as mentioned above, initially a parallel initiative was planned by the Scientific Director of CIHR’s Institute of Indigenous Peoples’ Health to focus on Indigenous peoples’ priorities for changing the health research ecosystem. Because of leadership changes within that institute, the parallel process was not undertaken to date. As such, although some Indigenous individuals participated in the surveys and knowledge exchange sessions described here and suggestions related to Indigenous health research were identified, this process was not led by Indigenous individuals. The suggestions related to Indigenous health research, which point to certain systemic changes that would facilitate Indigenous-led research, are included in this report and were provided to the Institute of Indigenous Peoples’ Health for their information. We hope that an Indigenous-led initiative occurs in the near future. Second, because of the timelines for this project, a rapid framework analysis was conducted; this method has been used extensively in qualitative research, including during the COVID-19 pandemic to meet timelines to inform decision making (Gale et al. 2019). Third, we focused the work on G7 countries, Australia, and New Zealand, which may have excluded promising initiatives from other countries. However, these countries were selected because of similarities in health research and health systems. Moreover, their inclusion is also a strength of the proposal in that the project looked outside of Canada for promising strategies. Fourth, given small cell numbers we are unable to report on intersections across participant demographics for all results. As such, we cannot comment on whether the participants in each project phase reflect the diversity of the population in Canada; however, we have diversity in province/territory representation and participant type.
There are several strengths to this initiative that make it unique. First, we used rigorous mixed methods to conduct this project, with each phase informing the next and engaging different cadres of knowledge users. Second, we conducted the sessions in English and French. We also optimized accessibility and engagement for participants across all data collection phases. Third, we included individuals from different interested parties including researcher leaders, researchers, funders, policy-makers, and members of the public. The inclusion of the latter group is a particular strength that makes this initiative unique from other research reviews. Given that members of the public are the intended focus of health research, it is critical that their views be incorporated. Fourth, we used trauma-informed approaches to engage the members of the public and ensured meetings and surveys were accessible.
In summary, we have a chance in Canada to reshape the health research system. The recommendations represent 12 actionable items for the post-pandemic advancement of Canada’s health research system, which will strengthen our health systems. While some of these actions are specific to pandemics or other emergencies, most focus on actions that should happen now and we risk much in Canada by not acting.
Acknowledgement
Sharon Straus holds a Tier 1 Canada Research Chair.
References
Andersen J.P., Nielsen M.W., Simone N.L., Lewiss R.E., Jagsi R. 2020. COVID-19 medical papers have fewer women first authors than expected. Elife, 9: e58807.
Audisio K., Lia H., Robinson N.B., Rahouma M., Soletti G. Jr, Cancelli G., et al. 2022. Impact of the COVID-19 pandemic on non-covid-19 clinical trials. Journal of Cardiovascular Development and Disease, 9(1): 19.
Bauchner H., Fontanarosa P.B., Golub R.M. 2020. Editorial evaluation and peer review during a pandemic: how journals maintain standards. Jama, 324(5): 453–454.
Breathe the Lung Association. n.d. Health charities call for relief as they support vulnerable Ontarians through COVID-19 [online]. Available from https://www.lung.ca/health-charities-call-relief-they-support-vulnerable-ontarians-through-covid-19 [accessed 22 January 2024].
Cai X., Fry C.V., Wagner C.S. 2021. International collaboration during the COVID-19 crisis: autumn 2020 developments. Scientometrics, 126(4): 3683–3692.
Caulfield T., Bubela T., Kimmelman J., Ravitsky V., 2021. Let’s do better: public representations of COVID-19 science. FACETS, 6: 403–423.
Davis P.B., Meagher E.A., Pomeroy C., Lowe W.L. Jr, Rubenstein A.H., Wu J.Y., et al. 2022. Pandemic-related barriers to the success of women in research: a framework for action. Nature Medicine, 28: 436–438.
Druedahl L.C., Minssen T., Nicholson Price W. 2021. Collaboration in times of crisis: a study on COVID-19 vaccine R&D Partnerships. Vaccine, 39(42): 6291–6295.
Fahim C., Cooper J., Theivendrampillai S., Pham Ba', Straus S. 2023. Ontarians’ perceptions of public health communications and misinformation during the COVID-19 pandemic: survey study. JMIR Formative Research, 7(e38323).
Fanning J.P., Murthy S., Obonyo N.G., Baillie J.K., Webb S., Dalton H.J., Fraser J.F. 2021. Global infectious disease research collaborations in crises: building capacity and inclusivity through cooperation. Globalization and Health, 17(1): 1–6.
G20 Research Group. 2020. G20 health ministers' declaration [online] Available from http://www.g20.utoronto.ca/2020/2020-g20-health-1119.html [accessed 22 January 2024].
Gale R.C., Wu J., Erhardt T., Bounthavong M., Reardon C.M., Damschroder L.J., Midboe A.M. 2019. Comparison of rapid vs in-depth qualitative analytic methods from a process evaluation of academic detailing in the veterans health administration. Implementation Science, 14(11).
Government of Canada. 2017. Canada's fundamental science review [online]. Available from https://ised-isde.canada.ca/site/canada-fundamental-science-review/en [accessed 22 January 2024].
Government of Canada. 2023. Report of the advisory panel on the federal research support system [online]. Available from https://ised-isde.canada.ca/site/panel-federal-research-support/sites/default/files/attachments/2023/Advisory-Panel-Research-2023.pdf [accessed 23 January 2024].
Halley M.C., Mathews K.S., Diamond L.C., Linos E., Sarkar U., Mangurian C., et al. 2021. The intersection of work and home challenges faced by physician mothers during the Coronavirus disease 2019 pandemic: a mixed-methods analysis. Journal of Women’s Health, 30(4): 514–524.
Hamilton A. 2013. Qualitative methods in rapid turn-around health services research [online]. Available from http://www.hsrd.research.va.gov/for_researchers/cyber_seminars/archives/video_archive.cfm?SessionID=780 [accessed 7 September 2022].
Hanney S.R., Straus S.E., Holmes B.J. 2022. Saving millions of lives but some resources squandered: emerging lessons from health research system pandemic achievements and challenges.Health Research Policy and Systems, 20.
Health Research Policy and Systems. 2021. The role of the health research system during the COVID-19 epidemic: experiences, challenges and future vision [online]. Available from https://www.biomedcentral.com/collections/HRPSCovid [accessed 22 January 2024].
HealthCareCAN. 2023. Submission to the standing committee on finance’s pre-budget consultations in advance of the 2024 federal budget [online]. Available from https://www.healthcarecan.ca/portfolio_item/submission-to-the-standing-committee-on-finances-pre-budget-consultations-in-advance-of-the-2024-federal-budget [accessed 22 January 2024].
Hoddinott S.N., Bass M.J. 1986. The Dillman total design survey method. Canadian Family Physician, 2366–2368.
Imagine Canada. 2021. New study: ongoing impacts of the COVID-19 crisis on the charitable sector [online]. Available from https://www.imaginecanada.ca/en/360/ongoing-impacts-covid-19-crisis-charitable-sector [accessed 22 January 2024].
Khazanchi R., Evans C.T., Marcelin J.R. 2020. Racism, not race, drives inequity across the COVID-19 Continuum. JAMA Network Open, 9(3).
Kowalski C. 2021. COVID has shown the power of science-industry collaboration. Nature, 594: 302.
Michael Smith Health Research BC. 2022. BC COVID-19 Strategic Research Advisory Committee Summary Report [online]. Available from https://healthresearchbc.ca/wp-content/uploads/2022/10/SRAC_Summary_Report_Oct2022.pdf [accessed 26 January 2024].
Michael Smith Health Research BC. 2023. 2023 British Columbia Health Research System Rapid Assessment [online]. Available from https://healthresearchbc.ca/wp-content/uploads/2023/12/2023_BC_Health_Research_System_Rapid_Assessment.pdf [accessed 26 January 2024].
Mishra S., Walker J.D., Wilhelm L., Larivière V., Bubela T., Strau S.E. 2023. Use and misuse of research: Canada's response to COVID-19 and its health inequalities. British Medical Journal, 382: e075666.
Myers K.R., Tham W.Y., Yin Y., Cohodes N., Thursby J.G., Thursby M.C., et al. 2020. Unequal effects of the COVID-19 pandemic on scientists. Nature Human Behaviour, 4: 880–883.
Narayana S., Roy B., Merriam S., Yecies E., Lee R.S., Mitchell J.L., Gottlieb A.S. 2020. Minding the gap: organizational strategies to promote gender equity in academic medicine during the COVID-19 pandemic. Journal of General Internal Medicine, 35(12): 3681–3684.
OECD. 2024. Gross domestic spending on R&D (indicator) [online]. Available from https://data.oecd.org/rd/gross-domestic-spending-on-r-d.htm [accessed 22 January 2024].
Palayew A., Norgaard O., Safreed-Harmon K., Andersen T.H., Rasmussen L.N., Lazarus J.V. 2020. Pandemic publishing poses a new COVID-19 challenge. Nature Human Behaviour, 4: 666–669.
Pang T., Sadana R., Hanney S., Bhutta Z.A., Hyder A.A., Simon J. 2003. Knowledge for better health: a conceptual framework and foundation for health research systems. Bulletin of the World Health Organization, 81(11): 815–820.
Rabinowitz L.G., Rabinowitz D.G. 2021. Women on the frontline: a changed workforce and the fight against COVID-19. Academic Medicine, 96(6): 808–812.
Saitz R., Schwitzer G. 2020. Communicating science in the time of a pandemic. Jama, 324(5): 443–444.
Staniscuaski F., Kmetzsch L., Soletti R.C., Reichert F., Zandonà E., Ludwig Z.M.C., et al. 2021. Gender, race and parenthood impact academic productivity during the COVID-19 pandemic: from survey to action. Frontiers in Psychology, 12(663252):.
The COVID-19 Immunity Task Force. 2021. The COVID-19 immunity task force [online]. Available from https://www.covid19immunitytaskforce.ca [accessed 22 January 2024].
Theivendrampillai S., Cooper J., Lee T., Lau M.W.K., Marquez C., Straus S.E., Fahim C. 2023. Canadian public perceptions and experiences with information during the COVID-19 pandemic: strategies to optimize future risk communications. BMC Public Health [Electronic Resource], 23(796): 1–12.
UK Covid-19 Inquiry. 2024. What is the UK COVID-19 inquiry? [online]. Available from https://covid19.public-inquiry.uk [accessed 22 January 2024].
UK Research and Innovation. 2023. Impact evaluation of UKRI’s R&I funding response to COVID-19 [online]. Available from https://www.ukri.org/publications/impact-evaluation-of-ukris-ri-funding-response-to-covid-19 [accessed 22 January 2024].
Appendix A. Definitions of the four functions of the WHO health research system framework
1.
Governance/stewardship including vision, priority setting, ethics, and monitoring/evaluation: being concerned with oversight of the entire health research system. It is primarily the responsibility of government, but others may have responsibility including national health research councils and professional associations. It includes four components: “definition and articulation of a vision for a national health research system; identification of appropriate health research priorities and coordination of adherence to them; setting and monitoring of ethical standards for health research and research partnerships; and monitoring and evaluation of the health research system itself (Pang et al. 2003)”.
2.
Financing: “securing of research funds and allocating these accountably” and subsequently monitoring these funds and allocation. This process should be efficient, transparent, and peer-review-based (Pang et al. 2003).
3.
Capacity building encompassing capacity to conduct (including supporting the life cycle of the researcher), receive, and use research: bringing new researchers and institutions into the health research system, further developing and sustaining the existent human and physical capacity, maintaining good physical facilities to conduct research, an attractive career structure, good research management, availability of funding, opportunities to present and discuss data, rapid access to current research information, and addressing internal or external researcher migration and “brain drain (Pang et al. 2003)”.
4.
Producing and using research to improve health and strengthen the public, social, and health care systems: “producing scientifically valid research outputs, translating, and communicating research to inform health policy, strategies, and practices, and public opinion, and promoting the use of research to develop new tools (drugs, vaccines, devices, and other applications) to improve health (Pang et al. 2003)”.
Appendix B. Knowledge exchange session discussion guide example
Knowledge exchange session 1 discussion guide
1. Knowledge translation (KT) program introduction (30 min)
Hello attendees, my name is [insert facilitator name] and I am [insert role and organization]. Thank you very much for agreeing to participate in this discussion and taking the time to speak with us. I also have [insert names of other team members] on the call with me today. The Knowledge Translation (KT) Program at St. Michael’s hospital is thrilled to be supporting this project. Please post in the chat or email Negin if you are having any technical issues.
1.1 Acknowledgement of traditional land
The KT Program is located on land now known as Tkaronto (Toronto). Tkaronto is the traditional territory of many groups, including the Mississaugas of the Credit and the Chippewa/Ojibwe of the Anishnaabe Nations; the Haudenosaunee; and the Wendat.
It is now home to many diverse First Nations, Inuit, and Métis peoples. We also acknowledge that Tkaronto is covered by Treaty 13 with the Mississaugas of the Credit and The Dish with One Spoon treaty between the Anishinaabe, Mississaugas, and Haudenosaunee that connected them to share the territory and protect the land.
We invite participants to share where they are located in the chat box.
1.2 Roundtable introductions and competing interests
We will now do quick introductions of everyone on the call. I will go through my list of names and call on you, please feel free to share your name, pronouns if you feel comfortable doing so, and your organization.
Additionally, thank you for providing any competing interests in advance through the survey. As a reminder, we sent these to all attendees. Before beginning, we want to provide opportunity to discuss these. Please feel free to share any competing interests, and any reflections on these.
1.3 Meeting agenda
1.
Framing for the discussion
2.
Review structure of the session
3.
Review survey results
4.
Review terms of consent
5.
Review survey results
6.
Small-group discussions
7.
Report back and large-group discussion
1.4 Purpose of this initiative
As a reminder, we are holding a series of sessions that are part of an international knowledge exchange initiative. Given the impact of the pandemic on health research systems worldwide, the purpose of this initiative is to develop actionable recommendations to strengthen Canada’s health research system post-pandemic. Please note that we are using Pang et al. (Pang et al. 2003) definition of a health research system, defined as the people, institutions, and activities whose primary purpose is to generate high-quality knowledge that can be used to promote, restore, and/or maintain the health status of populations.
We will be holding sessions with leaders from health research funding agencies and health, public health, and social care policy-makers, leaders from research institutes, and members of the public and researchers.
1.5 Purpose of today’s session
The purpose of this session specifically is to bring together leaders from health research funding agencies and health, public health, and social care policy-makers from G7 countries, Australia, and New Zealand to inform recommendations on strategies to strengthen the Canadian health research system and accelerate its post-pandemic recovery in the short, medium, and long-term; identify opportunities for collaboration on these strategies; and outline the potential consequences if these actions are not undertaken.
1.6 Structure of today’s session
We will be focusing our discussion today around four themes from the WHO research system framework (Pang et al. 2003); we will be defining these once we break out into our group discussions.
1.
Governance/stewardship including vision, priority setting, ethics, and monitoring/evaluation
2.
Financing
3.
Capacity building encompassing capacity to conduct (including supporting the life cycle of the researcher), receive, and use research
4.
Producing and using research to improve health and strengthen the public, social, and health care systems
For today’s session, we will focus on the following overarching questions, to be addressed within each of the four themes.
1.
What did you do in this area and why?
2.
Did it work—why/why not?
3.
What do you wish you’d done differently and why?
Think about what you did at the beginning of the pandemic and how that has evolved through subsequent waves and now into recovery.
The structure of today’s session will include small- and large-group discussions. We will assign everyone to a breakout room to discuss in small groups these three questions, within each of the four themes. The small groups will last 1 h. Following this, we will come back to the large group to report back and continue discussion. The large-group discussion will last about 1 h and 15 min. This session will last approximately 3 h total.
There will be a facilitator in each small group to lead the discussion.
Please feel free to post any suggestions in the chat during both the large- and small-group discussions. We will make sure to save the chat and include it in our analysis.
Please note that we will record and transcribe both the small- and large-group discussions.
Before we break out into rooms, here are some guidelines for today’s session:
1.
We strongly urge you to respect each other’s privacy and not discuss who participated or what is said in the discussion with others.
2.
To allow us to capture all the information being discussed today as a group, we would request that everyone say their name and organization before they speak and take turns speaking to avoid speaking at the same time. Please note that we will ask you to repeat your name following your comment if you have not provided it.
3.
If we have not heard you respond for a few questions, we may call on you to encourage you to provide an answer. Please feel free to decline answering any question you would not like to provide an answer for.
4.
We also want to emphasize there is no need to wait for the facilitator to call on you to speak, feel free to jump in once the other person is done talking.
1.7 Overview of survey results
Thank you for completing the survey and providing, in advance, strategies your organization is using to strengthen health research systems within these four themes. Below and in our break out groups, we will share the results of the survey. We hope this will act as a launch point for today’s discussion. [Summary to be included in slides].
1.8 Terms of consent
As a reminder, the email inviting you to this session outlined the terms of consent for participation. These are also included in the meeting package attached to the meeting invite. I will run through them briefly again before we begin.
1.
Your participation is voluntary.
2.
You can choose to stop participating at any time.
3.
No one other than the research team, the transcriptionist, project partners, and other individuals participating in this session with you will know what you said.
4.
The session will be recorded. Participants can leave their cameras on or off.
5.
Any identifiable information, with the exception of your professional role type, will be omitted during transcription.
6.
The session results will be pooled and reported without any personal information in publicly available products; though we may include your organization type (e.g., “a provincial health research organization”). De-identified quotes may be used in reports and publications.
7.
Participants are free to contact the study team and withdraw their data prior to the data analysis stage.
8.
If you do not consent to participate, please feel free to disconnect from the call. Your consent to participate will be implied by staying on the line.
Are there any questions before we begin?
1.9 Break out room preparation
We have split you into two groups. Group 1 will stay in this main room, and Group 2 will go into the breakout room. I will now list off who is in each room. Again, if you are in Group 1, please remain here in the main room. If you are in Group 2, please enter into the breakout room when prompted.
*Group 2 departs into the breakout room*
2. Survey results and small-group discussion questions (60 min)
We will now begin recording.
*Begin recording session*
We will now get started with the questions…
| Theme 1—governance/stewardship including vision, priority setting, ethics, and monitoring/evaluation | |
1. The first theme we will discuss is governance/stewardship. Pang et al. (Pang et al. 2003) define governance/stewardship as being concerned with oversight of the entire health research system. It is primarily the responsibility of government, but others may have responsibility including national health research councils and professional associations. It includes four components: “definition and articulation of a vision for a national health research system; identification of appropriate health research priorities and coordination of adherence to them; setting and monitoring of ethical standards for health research and research partnerships; and monitoring and evaluation of the health research system itself”. 2. Survey respondents were asked how the strategies have been modified to support pandemic recovery: | |
| Modification | Number of participants |
| Identified and incorporated key COVID-19 related goals and priorities into organizational plans | 11 |
| Developed new projects and programs to study the impacts of COVID-19 | 6 |
| Created new teams and linkages both internal and external to the organization | 3 |
| Implemented virtual processes to replace in-person processes | 2 |
| New or increased organizational focus on health equity | 2 |
1. Discussion questions: • What did you do in this area and why? • Did it work—why/why not? • What do you wish you’d done differently and why? 2. Think about what you did at the beginning of the pandemic and how that has evolved through subsequent waves and now into recovery | |
| Theme 2—financing | |
1. The second theme we will discuss is financing. According to Pang et al. (Pang et al. 2003) financing of health research systems refers to “securing of research funds and allocating these accountably” and subsequently monitoring these funds and allocation. This process should be efficient, transparent, and peer-review-based. 2. Survey respondents were asked how the strategies have been modified to support pandemic recovery: | |
| Modification | Number of participants |
| Changed priorities of funded research to focus on COVID-19 recovery and broader long-term impacts of COVID-19 | 6 |
| Increasing amount and accessibility of funding for COVID-19 research | 7 |
| Tracking COVID-19 research funding allocation and needs | 2 |
1. Discussion questions: • What did you do in this area and why? • Did it work—why/why not? • What do you wish you’d done differently and why? 2. Think about what you did at the beginning of the pandemic and how that has evolved through subsequent waves and now into recovery | |
| Theme 3—capacity building encompassing capacity to conduct (including supporting the life cycle of the researcher), receive, and use research | |
1. The third theme we will discuss is capacity building, encompassing capacity to conduct (including supporting the life cycle of the researcher), receive, and use research. Pang et al. (Pang et al. 2003) define this as bringing new researchers and institutions into the health research system, further developing and sustaining the existent human and physical capacity, maintaining good physical facilities to conduct research, an attractive career structure, good research management, availability of funding, opportunities to present and discuss data, rapid access to current research information, and addressing internal or external researcher migration and “brain drain”. 2. Survey respondents were asked how the strategies have been modified to support pandemic recovery: | |
| Modification | Number of participants |
| Supported staff and researchers based on their needs | 6 |
| Developed infrastructure and staff positions to support COVID-19 recovery | 9 |
| Modified format and timelines of capacity-building programs | 3 |
| Downsized research work to support other COVID-19 efforts | 2 |
1. Discussion questions: • What did you do in this area and why? • Did it work—why/why not? • What do you wish you’d done differently and why? 2. Think about what you did at the beginning of the pandemic and how that has evolved through subsequent waves and now into recovery | |
| Theme 4—producing and using research to improve health and strengthen the public, social, and health care systems | |
1. The fourth theme we will discuss is producing and using research to improve health and strengthen the public, social, and health care systems. Pang et al. (Pang et al. 2003) define this as “producing scientifically valid research outputs, translating and communicating research to inform health policy, strategies, and practices, and public opinion, and promoting the use of research to develop new tools (drugs, vaccines, devices and other applications) to improve health”. 2. Survey respondents were asked how the strategies have been modified to support pandemic recovery: | |
| Modification | Number of participants |
| Held COVID-19-related knowledge translation events | 5 |
| Developed COVID-19-related knowledge translation materials | 5 |
| Supported partnerships and integrated knowledge translation activities | 4 |
| Modified formats of knowledge translation events | 3 |
| Developed new methods to share data | 1 |
| Attention to equity, diversity, inclusion, and racism in knowledge mobilization activities | 1 |
1. Discussion questions: • What did you do in this area and why? • Did it work—why/why not? • What do you wish you’d done differently and why? 2. Think about what you did at the beginning of the pandemic and how that has evolved through subsequent waves and now into recovery | |
3. Break (10 min)
We will now take a 10 min break. Please come back by [insert time]. Once we are all back we will share what we talked about in our breakout rooms and have more discussion.
4. Report back in large group and discussion (1 h and 15 min)
We will now go through each of the themes and will briefly summarize the small-group discussions, and following each summary, we will provide a chance for the group to discuss these further, with some prompting questions.
| Theme 1—governance/stewardship including vision, priority setting, ethics, and monitoring/evaluation |
| Areas of focus: 1. Organizational focus on health equity a. And in general, how was equity, diversity, and inclusion (EDI) considered/not considered? 2. Coordination of research/research funding/research initiatives 3. What was the balance of Covid/non-Covid research/capacity building considerations? 4. Was there a benefit of centralization of priority setting of research? And what were the pros/cons? |
| Theme 2—financing |
| Areas of focus: 1. Coordination of funding and avoiding duplication of effort 2. Sustainability of initiatives, including research networks, funding 3. How was EDI considered/not considered? 4. What was the balance of Covid/non-Covid research/capacity building considerations? 5. Was there a benefit of centralization of priority setting of research? And what were the pros/cons? |
| Theme 3—capacity building encompassing capacity to conduct (including supporting the life cycle of the researcher), receive, and use research |
| Areas of focus: 1. Retaining and sustaining a workforce 2. Gaps in training/paths for researchers 3. How was EDI considered/not considered? 4. What was the balance of Covid/non-Covid research/capacity building considerations? 5. Was there a benefit of centralization of priority setting of research? And what were the pros/cons? |
| Theme 4—producing and using research to improve health and strengthen the public, social, and health care systems |
| Areas of focus: 1. What happens next? How do we sustain/scale/spread? 2. How was EDI considered/not considered? 3. What was the balance of Covid/non-Covid research/capacity building considerations? 4. Was there a benefit of centralization of priority setting of research? And what were the pros/cons? |
5. Next steps (3 min)
Next steps:
1.
We are holding session 2 with leaders from health research organizations on 26 October 2022
2.
We are holding session 3 with members of the public and researchers in the coming months
3.
Based on these three sessions, we will be developing recommendations to strengthen Canada’s health research system post-pandemic: winter/spring 2023
4.
We will be sending around a survey for input on the draft recommendations: winter/spring 2023
6. Thank you! (3 min)
Thank you for taking the time to take part in this session. For questions or additional comments please contact [insert email]. If you have any follow up comments, please feel free to share them by email by 28 October 2022.
Appendix C. Surveys
Survey 1
Q1 Background
The Royal Society of Canada Working Group on Health Research System Recovery, in partnership with the Canadian Institutes of Health Research (CIHR), is holding a series of sessions that are part of an international knowledge exchange initiative. Given the impact of the COVID-19 pandemic on health research systems worldwide, the purpose of this initiative is to develop actionable recommendations to strengthen Canada’s health research system post-pandemic. Health research system can be defined as the people, institutions, and activities whose primary purpose is to generate high-quality knowledge that can be used to promote, restore, and/or maintain the health status of populations.
We will be holding sessions with leaders from health research funding agencies; health, public health, and social care policy-makers; leaders from research institutes; individual researchers; and members of the public.
In preparation for these meetings with representatives from organizations and sectors such as yours, we are requesting your completion of this survey to
•
Outline strategies within your organization that address any of the four themes from the WHO research system framework 1 (listed below)
•
Indicate whether these strategies have been modified to support pandemic recovery
•
Declare any competing interests
Themes from the WHO research system framework (Pang et al. 2003):
1.
Governance/stewardship including vision, priority setting, ethics, and monitoring/evaluation
2.
Financing
3.
Capacity building encompassing capacity to conduct (including supporting the life cycle of the researcher), receive, and use research
4.
Producing and using research to improve health and strengthen the public, social, and health care systems
Q2 Terms of consent
Before beginning the survey, please review the terms of consent. If you have any questions please contact [email protected].
•
Your participation in this survey is voluntary.
•
You can choose to stop completing the survey at any time, though any responses up to that point may be used, as outlined below.
•
The responses will be synthesized by relevant members of the KT Program, Unity Health Toronto.
•
Prior to the sessions we will disseminate information on reported strategies collected from the survey and any supporting documents provided, to session participants.
•
The results of the survey will also help form the recommendations.
•
Results will be pooled and may be publicly reported in products summarizing the results (e.g., reports and publications), without any personal information, though we may include your organization type (e.g., “a provincial health research organization”). De-identified quotes may be used in reports and publications.
•
There is minimal risk associated with participation in this study; however, there is a risk that participants may later regret sharing some responses in the survey; however, participants are free to contact the study team and withdraw their data prior to the data analysis stage. As it is possible that participants may disclose identifying information, all such identifying information will be changed in any written reports or oral presentations so that participants’ privacy will be protected.
•
If you consent to the terms of the study you are welcome to begin. Your consent to participate will be implied by beginning the survey.
Q3 Name:
Q4 Email:
Q5 Organization name:
Q6 Department:
Q7 Job title:
Q8 Organization size:
◯ Small (1 to 99 employees)
◯ Medium (100 to 499 employees)
◯ Large (500 employees or more)
◯ Unsure
Q9 Age of organization:
◯ Less than 10 years
◯ 10 to 20 years
◯ 21 to 30 years
◯ Greater than 30 years
◯ Unsure
Q10 Please select the term that best describes your organization as a stakeholder:
◯ Health research funding agency
◯ Research organization
◯ Research user
◯ Other _______________________________________________
Display this question:
Please select the term that best describes your organization as a stakeholder: = Health research funding agency
Q11 Please select the type of health research funding agency:
◯ Not for profit
◯ Charity
◯ Government
◯ Industry
◯ Other_______________________________________________
Display this question:
Please select the term that best describes your organization as a stakeholder: = Research organization
Q12 Please select the type of research organization:
◯ University
◯ University-affiliated research institute
◯ Government
◯ Non-governmental organization
◯ Other_______________________________________________
Display this question:
Please select the term that best describes your organization as a stakeholder: = Research user
Q13 Please select the type of research user:
◯ Government
◯ Journal
◯ Other _______________________________________________
Q14 Theme 1—governance/stewardship including vision, priority setting, ethics, and monitoring/evaluation.
Pang et al. (Pang et al. 2003) define governance/stewardship as being concerned with oversight of the entire health research system. It is primarily the responsibility of government, but others may have responsibility including national health research councils and professional associations. It includes four components: “definition and articulation of a vision for a national health research system; identification of appropriate health research priorities and coordination of adherence to them; setting and monitoring of ethical standards for health research and research partnerships; and monitoring and evaluation of the health research system itself”.
Q15 With this definition in mind, please briefly list any strategies your organization implemented that address this theme (e.g., development of a plan with indicators to evaluate implementation of your organizations’ funded research) or provide links to any relevant material on your website describing these strategies or send them to [email protected]. Alternatively, feel free to contact us to set up a brief phone call to provide this information. We anticipate that some of the strategies might be at the initial implementation phases, while others may be in implementation planning stages.
Q16 Have the strategies been modified to support pandemic recovery?
◯ Yes
◯ No
Display this question:
If Have the strategies been modified to support pandemic recovery? = Yes
Q17 If yes, how has your organization modified the strategies? Alternatively, feel free to send relevant links/information to [email protected] or contact us to set up a brief phone call to provide this information.
Q18 Theme 2—financing According to Pang et al. (Pang et al. 2003) financing of health research systems refers to “securing of research funds and allocating these accountably” and subsequently monitoring these funds and allocation. This process should be efficient, transparent, and peer-review-based.
Q19 With this definition in mind, please briefly list any strategies your organization implemented that address this theme (e.g., allocating research funds to COVID-related research) or provide links to any relevant material on your website describing these strategies or send them to [email protected]. Alternatively, feel free to contact us to set up a brief call to provide this information. We anticipate that some of the strategies might be at the initial implementation phases, while others may be in implementation planning stages.
Q20 Have the strategies been modified to support pandemic recovery?
◯ Yes
◯ No
Display this question:
If Have the strategies been modified to support pandemic recovery? = Yes
Q21 If yes, how has your organization modified the strategies? Alternatively, feel free to send relevant links/information to [email protected] or contact us to set up a brief phone call to provide this information.
Q22 Theme 3—Capacity building
Capacity building can encompass capacity to conduct (including supporting the life cycle of the researcher), receive, and use research. Pang et al. (Pang et al. 2003) define this as bringing new researchers and institutions into the health research system, further developing and sustaining the existent human and physical capacity, maintaining good physical facilities to conduct research, an attractive career structure, good research management, availability of funding, opportunities to present and discuss data, rapid access to current research information, and addressing internal or external researcher migration and “brain drain”.
Q23 With this definition in mind, please briefly list any strategies your organization implemented that address this theme (e.g., offering research staff trainings on novel research methods) or provide links to any relevant material on your website describing these strategies or send them to [email protected]. Alternatively, feel free to contact us to set up a brief call to provide this information. We anticipate that some of the strategies might be at the initial implementation phases, while others may be in implementation planning stages.
Q24 Have the strategies been modified to support pandemic recovery?
◯ Yes
◯ No
Display this question:
If Have the strategies been modified to support pandemic recovery? = Yes
Q25 If yes, how has your organization modified the strategies? Alternatively, feel free to send relevant links/information to [email protected] or contact us to set up a brief phone call to provide this information.
Q26 Theme 4—producing and using research to improve health and strengthen the public, social, and health care systems
Pang et al. (Pang et al. 2003) define this as “producing scientifically valid research outputs, translating and communicating research to inform health policy, strategies, and practices, and public opinion, and promoting the use of research to develop new tools (drugs, vaccines, devices, and other applications) to improve health”.
Q27 With this definition in mind, please briefly list any strategies your organization implemented that address this theme (e.g., holding knowledge exchange events with researchers and policy-makers who may use the research) or provide links to any relevant material on your website describing these strategies or send them to [email protected]. Alternatively, feel free to contact us to set up a brief call to provide this information. We anticipate that some of the strategies might be at the initial implementation phases, while others may be in implementation planning stages.
Q28 Have the strategies been modified to support pandemic recovery?
◯ Yes
◯ No
Display this question:
If Have the strategies been modified to support pandemic recovery? = Yes
Q29 If yes, how has your organization modified the strategies? Alternatively, feel free to send relevant links/information to [email protected] or contact us to set up a brief phone call to provide this information.
Q30 Competing interests Competing interests can take several forms including financial, business/professional, intellectual, affiliations, or memberships in associations, research funding, payments, gifts, gratuities, honoraria, advocacy, consulting, and others.
Q31 Are you involved in any activities that could create real, potential, or apparent conflicts of interest that could affect your responses in this survey or in the upcoming session (if attending)? Please note that for transparency, your name along with your competing interests will be shared with session participants before the session.
◯ Yes
◯ No
Display this question:
If Are you involved in any activities that could create real, potential, or apparent conflicts of in… = Yes
Q32 If yes, please describe
Survey 2
Q1 Background
The Royal Society of Canada Working Group on Health Research System Recovery, along with the Canadian Institutes of Health Research (CIHR) held a series of sessions that were part of an international knowledge exchange initiative. Given the impact of the pandemic on health research systems worldwide, the purpose of this initiative was to develop actionable recommendations to strengthen Canada’s health research system post-pandemic.
The World Health Organization (WHO) defines a health research system as “the people, institutions, and activities whose primary purpose in relation to research is to generate high-quality knowledge that can be used to promote, restore, and/or maintain the health status of populations; it should include the mechanisms adopted to encourage the utilization of research” (Pang et al. 2003).
The WHO Health Research Ecosystem Framework includes four components:
1.
Governance/stewardship, which includes coordination, priority setting, ethics, monitoring, evaluation, and accountability
2.
Financing, which includes securing and allocating funding with accountability and transparency
3.
Capacity building, which includes human and physical capacity to conduct, absorb, and use health research
4.
Producing and using research, which includes producing, promoting, disseminating, and implementing research in practice, policy, and public opinion
To develop these recommendations, we held sessions with national and international leaders from health research funding agencies; health, public health, and social care policy-makers; leaders from research institutes; individual researchers; and members of the public. We also contextualized the recommendations using input from the recently released report of the Advisory Panel on the Federal Research Support System.
Through this survey, we are requesting your feedback on these recommendations, which will then be disseminated broadly to all relevant organizations (e.g., funders, government, research organizations).
This survey will take 15–20 min to complete.
Q2 Terms of consent
Before beginning the survey, please review the terms of consent. If you have any questions please contact Robyn Beckett at [email protected].
•
Your participation in this survey is voluntary.
•
You can choose to stop completing the survey at any time, though any responses up to that point may be used, as outlined below.
•
No one other than the research team will know what you responded.
•
Your responses will be compiled by relevant members of the Knowledge Translation Program, Unity Health Toronto.
•
The results will help refine the recommendations. Results will be pooled and may be publicly reported in products summarizing the results (e.g., reports and publications), without any personal information, though we may include your organization type (e.g., “a provincial health research organization”). De-identified quotes may be used in reports and publications.
•
There is minimal risk associated with participation in this study. Minor risks include (1) participants may later regret sharing some responses in the survey; however, participants are free to contact the study team and withdraw their data prior to the data analysis stage; and (2) in the feedback section participants may disclose identifying information; however, all such identifying information will be changed in any written reports or oral presentations so that participants’ privacy will be protected.
•
If you consent to the terms of the study you are welcome to begin. Your consent to participate will be implied by beginning the survey.
Q3 Please select the term(s) that best describe your organization or you as a stakeholder (select all that apply):
□ Health research funding agency
□ Research organization
□ Research user (e.g., member of the public or patient, government employee, journal staff, and healthcare provider)
□ Other_______________________________________________
Display this question:
Please select the term(s) that best describe your organization or you as a stakeholder (select all that apply): = Health research funding agency
Q4 Please select the type of health research funding agency (select all that apply):
□ Not for profit
□ Charity
□ Government
□ Industry
□ Other_______________________________________________
Display this question:
Please select the term(s) that best describe your organization or you as a stakeholder (select all that apply): = Research organization".
Q5 Please select the type of research organization (select all that apply):
□ University
□ University-affiliated research institute
□ Government
□ Non-governmental organization
□ Other_______________________________________________
Display this question:
Please select the term(s) that best describe your organization or you as a stakeholder (select all that apply): = Research user (e.g., member of the public or patient, government employee, journal staff, and healthcare provider).
Q6 Please select the type of research user (select all that apply):
□ Government employee
□ Journal staff
□ Clinician/healthcare provider
□ Health care manager
□ Member of the public or patient
□ Other_______________________________________________
Q7 The next several pages provide the recommendations organized by the four themes from the World Health Organization’s health research systems framework (governance/stewardship, financing, capacity building, and producing and using research). Please rate each recommendation on the importance for implementation in Canada on a scale from 1 to 9, with 1 being not at all important, 5 being moderately important, and 9 being extremely important. Please also provide any comments or suggestions for the recommendations in the open text boxes. These questions may be repetitive, but we appreciate your feedback across all the recommendations. Note that you can click on the hyperlinked terms in some of the statements to obtain definitions/more information.
Q8 Theme 1: governance/stewardship
Q9 Coordinate research efforts across local, provincial, national, and international entities. Specifically:
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| Leverage and extend the use of the Canada Research Coordinating Committee (CRCC) across the TriCouncil Agencies and the Canada Foundation for Innovation (CFI) to provide research and innovation advice, oversight, coordination, and communication across the TriCouncil Agencies. Please click on the organization/project names to learn more. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Create a new entity, entitled the Canadian Knowledge and Science Foundation (CKSF) to rapidly address emerging research and innovation needs, deliver TriCouncil Agency programming, and enhance coordination, planning, and policy capacity across the research support system (as suggested in the recent report of the Advisory Panel on the Federal Research Support System) | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Establish a health research funding agency in each province/territory through which the provincial/territorial health ministry and public health agency can connect on research priorities and evidence needs | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Establish a structure whereby the Public Health Agency of Canada and Health Canada connect with provincial/territorial health research agencies and provincial/territorial ministries responsible for health and public health on research priorities and evidence needs | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
Q10 Please provide any comments or suggestions for the above set of recommendations.
Q11 Theme 1: Governance/stewardship
Q12 Create communications infrastructure. Specifically:
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| Through regular and frequent meetings, promote coordination and communication between the Canadian Institutes of Health Research (CIHR) and Health Canada to facilitate research conduct, use, and funding | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Through regular meetings, promote coordination and communication between federal and provincial/territorial funders and relevant federal and provincial policy-makers (e.g., the National Alliance of Provincial Health Research Organizations (NAPHRO)) to align and facilitate research conduct and use | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Develop centralized processes to communicate and coordinate research priorities with knowledge users (such as researchers, academic institutions, charitable organizations, and patient/public organizations including equity-deserving groups) | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Establish a communication platform to outline what research questions/priorities different funders (e.g., provincial/territorial, TriCouncil Agencies) are responsible for to limit duplication and support replication | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Encourage the use of communication platforms between TriCouncil Agencies and international funding agencies to align research priorities in pandemics/health emergencies to coordinate research (e.g., Global Research Collaboration for Infectious Disease Preparedness (GloPID-R)) | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Develop principles of transparent communication around what research is funded | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Develop and publicly report data on research impact and overall impact of research funding | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
Q13 Please provide any comments or suggestions for the above set of recommendations.
Q14 Theme 1: governance/stewardship.
Q15 Outline research logistics as a part of emergency preparedness. Specifically:
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| Create an emergency preparedness research plan that includes data sharing, cybersecurity, research ethics board (REB) approvals, and supply chain procedures | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Ensure the emergency preparedness research plan includes the coordination of research questions with international research funders to prioritize based on capacity, expertise, and infrastructure | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Develop data sharing agreements within and across provinces/territories and between provinces/territories and national partners (e.g., Canadian Institute for Health Information (CIHI)) for sharing data including health research, health services, and registry data | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Centralize and harmonize research ethics board (REB) processes nationally with a single online form, standardized training, and tracking of timelines | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Prioritize REB for relevant studies during health/public health emergencies | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Harmonize processes (including data collection, privacy, and REB) for biobanks and data sharing within provinces/territories and across provinces/territories to facilitate rapid research | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
Q16 Please provide any comments or suggestions for the above set of recommendations.
Q17 Theme 1: governance/stewardship
Q18 Prioritize equity in research processes. Specifically:
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| Use equity and anti-oppression principles in all governance decision making and actions aligned with the TriCouncil Agency’s Dimensions Charter and the rights of First Nations, Inuit, and Métis Peoples | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Include patients/public at all governance levels in the health research ecosystem using an open, transparent recruitment process and publicly report on their inclusion | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Sustain Indigenous-led biobanks and data sharing | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Create national database of ongoing studies for patients to engage with as research partners and research leads | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
Q19 Please provide any comments or suggestions for the above set of recommendations.
Q20 Theme 1: governance/stewardship
Q21 Facilitate streamlined, inclusive grant review process. Specifically:
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| Monitor grant application and success rates by applicants’ PROGRESS PLUS factors (an acronym used to identify characteristics that stratify health opportunities and outcomes) and report on this information publicly | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Ensure equity and diversity principles are embedded within all grant applications, including the consideration that research team and patient partners should reflect the diversity of relevant population | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Reimburse peer reviewers for any caregiving support required for their dependents, to enable the peer reviewers to attend meetings | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Mandate that principal investigators with peer-reviewed grants must participate in grant peer review for the duration of their grant support | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Use the grant application and success data to revise grant competitions (e.g., to prioritize specific research areas, researchers from equity-deserving groups, etc.) | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Standardize virtual and hybrid processes for grant peer review | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Include patients in grant peer review process | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Use Public Health Agency of Canada’s Strengthening the Integration of Intersectionality Theory in Health Inequality Checklist when reviewing grants to assess if and how they adhere to equity considerations | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Create multidisciplinary grant review panels and provide peer review training for multidisciplinary research | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Create iterative grant peer review process with opportunity for interviews with applicants and peer review panel to clarify questions/responses | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Streamline the grants application process for patients such as reducing requirements for patients to complete letters of support, CVs and sex- and gender-based analysis plus (GBA+) modules (e.g., Women’s College Research Institute’s (WCRI) GBA+) | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Conduct peer review of the grant peer review process (including peer reviewers) and make results of this peer review transparent | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
Q22 Please provide any comments or suggestions for the above set of recommendations.
Q23 Theme 2: financing
Q24 Reimagine funding of research. Specifically:
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| Embed equity considerations in decision making on all research investments | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Ensure long-term funding for successful research enterprises and develop strategies for defunding initiatives that aren't achieving relevant impact | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Assess extent to which research infrastructure and research infrastructure funding exists for therapeutics, vaccine, diagnostic testing development and implementation | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Establish funding for provincial/territorial health research hubs with linkages to health, public health, social care, education and cross-disciplinary collaborations (e.g., National Institute for Health and Care Research (NIHR) Clinical Research Networks, Applied Research Collaborations, National Health and Medical Research Council (NHMRC) Translational Research Centres, National Institutes of Health (NIH) Implementation/translation Research Centres) | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Develop strategies for sustainability of networks/platforms/hubs through partnerships with national/provincial/territorial funders | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Increase overhead/indirect cost allowance (cost of doing research including space, human resources, contracts support) for research institutes to 50% to completely cover cost of research operations | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Engage with industry to contribute to funding for health research hubs/networks/platforms | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Work with industry to provide unrestricted funds for project research grants and infrastructure grants | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Make research funding allocations transparent, and report on the distribution of funding by applicants’ PROGRESS PLUS factors (e.g., gender, race) | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Make a clear separation between knowledge user-driven versus researcher-driven research; have separate funding for both groups | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Support mechanisms for crowdfunding research | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
Q25 Please provide any comments or suggestions for the above set of recommendations.
Q26 Theme 2: financing
Q27 Support researchers. Specifically:
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| Develop collaborative grants across the TriCouncil Agencies that support cross-disciplinary training of PhD students and post-doctoral fellows | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Create salary support pathways for scientists (such as salary support awards or embedding salary into grants) throughout their career trajectories from early career to mid- and senior-career | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Create similar salary support pathways for clinician scientists throughout their career trajectories from early career to mid- and senior-career | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Expand joint industry/academic and PhD/post-doctoral training opportunities | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Expand joint government/academic training opportunities for PhD/post-doctoral trainees | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Establish and maintain living wage standards for salaries for graduate students and post-doctoral fellows | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
Q28 Please provide any comments or suggestions for the above set of recommendations.
Q29 Theme 3: capacity building
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| Embed equity, diversity, and anti-racism principles in all research capacity-building activities | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Create opportunities for Postdoctoral Fellowships across academia, industry, and government sectors | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Create opportunities for Postdoctoral Fellows to work in more than one sector (academic, industry, or government) during a fellowship | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Use provincial/territorial/national data to estimate needs for the health human workforce and the research workforce using dynamic modelling (e.g., align training opportunities while monitoring for burnout/lack of retention) | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Create transdisciplinary research training networks for graduate students, fellows and early career researchers to facilitate research and research training in diverse methods and disciplines across all research pillars (e.g., implementation science, one health, artificial intelligence (AI)) | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Create support strategies for those disproportionately affected systematically and during the pandemic such as Black, Indigenous, and people of colour, women, non-binary people, and clinician scientists | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Provide training for researchers on trauma-informed approaches to patient engagement; that is, approaches rooted in an understanding of how trauma impacts people, with the purpose of avoiding potential re-traumatization during the research process. These approaches also acknowledge broader social contexts and how systems of oppression (e.g., colonialism, white supremacy) cause trauma. | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Ensure patient engagement in research uses trauma-informed approaches | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Provide training for researchers, patient partners, and policy-makers on anti-oppression practices in research; that is, practices that name and seek to dismantle injustices and power imbalances in the broader social context and in the research processes (e.g., asking community members most impacted by the research to lead key research activities such as developing the project plan and the budget). | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Provide training for researchers, patients, and policy-makers on knowledge mobilization | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
Q31 Please provide any comments or suggestions for the above set of recommendations.
Q32 Theme 4: producing and using research
Q33 Producing research
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| Create a network of chief science advisors in each national/provincial/territorial government department Create opportunities for these advisors via knowledge exchange with researchers across Canada These advisors can interpret and communicate science to policy-makers including communication of evidence uncertainty | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Create funding opportunities such as partnership grants between researchers and knowledge users to focus on research uptake | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Further develop multidisciplinary, collaborative grants across the TriCouncil Agencies (leveraging New Frontiers in Research Fund) that support collaborations across research disciplines including those that range from developing the team/research project through to completion of research and its dissemination | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Create health research hubs within provinces/territories to link health care delivery context with research across all Canadian Institutes of Health Research (CIHR) pillars; include patient/public engagement and commercialization | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Create a national network of the provincial/territorial health research hubs and identify focused areas (e.g., methodological, clinical) that each may lead/co-lead nationally (for example, in areas such as pandemic preparedness, healthy aging, climate change, one health, health/social disparities, artificial intelligence (AI) innovation, patient/public engagement, implementation science/knowledge mobilization) | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Embed clinical trials platform(s) within health care delivery/health research hubs | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
Q34 Please provide any comments or suggestions for the above set of recommendations.
Q35 Theme 4: producing and using research
Q36 Using research
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|
| Enhance science to policy dissemination training for researchers (e.g., in plain language communication) through various approaches including modules and embedded training opportunities | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Enhance science to policy dissemination training for policy-makers (e.g., in plain language communication) through various approaches including modules and embedded training opportunities | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Co-create and deliver public education strategies for increasing health research literacy with members of the public | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Co-create and deliver training for patients on engaging in research | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Co-create and deliver training for patients on interacting with policy-makers | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
| Create communication/knowledge exchange opportunities across funded networks/platforms/hubs | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ | ◯ |
Q37 Please provide any comments or suggestions for the above set of recommendations.
Q38 Is there anything not captured in this list of recommendations that should be added?
Survey 3
Q1 Background
Thank you for your interest in the international knowledge exchange initiative led by the Royal Society of Canada Working Group on Health Research System Recovery, and in partnership with the Canadian Institutes of Health Research (CIHR). We held sessions with leaders from health research funding agencies; health, public health, and social care policy-makers; leaders from research institutes; individual researchers; and members of the public to develop a set of actionable recommendations to strengthen Canada’s health research system post-pandemic. After receiving public input, we developed and refined these recommendations. The updated version of the recommendations is provided in this survey.
There are reviews underway at the national and provincial/territorial levels into the COVID-19 research response and this work will feed into and benefit those reviews. The responses from this survey will be used to select one priority example across each category and present this to a wide range of executive decision-makers as a priority focus. We will be preparing a document with the list of recommendations and a description of some specific examples of what could be implemented and by whom. This document will be shared by the Canadian Institutes of Health Research (CIHR) and the Royal Society of Canada with relevant partners.
In this survey, there are 12 recommendations; each is followed by some specific examples of how these recommendations could be implemented and by whom. For each recommendation, we ask that you let us know which specific examples you think should be prioritized for implementation. For each of your selections, we ask you to specify who should be responsible for implementing it. We also invite you to provide any final suggestions to the wording of the 12 recommendations and examples.
This survey may take 15–20 min to complete; you may come back and resume the survey using the initial link.
Q2 Terms of consent
Before beginning the survey, please review the terms of consent. If you have any questions please contact Robyn Beckett at [email protected].
•
Your participation in this survey is voluntary.
•
You can choose to stop completing the survey at any time, though any responses up to that point may be used, as outlined below.
•
No one other than the research team will know what you responded.
•
Your responses will be compiled by relevant members of the Knowledge Translation Program, Unity Health Toronto.
•
Results will be pooled and may be publicly reported in products summarizing the results (e.g., reports, publications), without any personal information, though we may include your organization type (e.g., “a provincial health research organization”). De-identified quotes may be used in reports and publications.
•
There is minimal risk associated with participation in this study. Minor risks include (1) participants may later regret sharing some responses in the survey; however, participants are free to contact the study team and withdraw their data prior to the data analysis stage; and (2) in the feedback section participants may disclose identifying information; however, all such identifying information will be changed in any written reports or oral presentations so that participants’ privacy will be protected.
•
If you consent to the terms of the study you are welcome to begin. Your consent to participate will be implied by beginning the survey.
Q3 Organization name (if applicable):
Q4 Department (if applicable):
Q5 Job title (if applicable)
Q6 Please select the term(s) that best describe your organization or you as a stakeholder (if applicable) (select all that apply):
□ Health research funding agency (includes foundations that fund health research (e.g., Health Research BC))
□ Government (e.g., Ministry of Health)
□ Research organization
□ Research user (e.g., member of the public or patient, government employee, journal staff, and healthcare provider)
□ Other _______________________________________________
Display this question:
Please select the term(s) that best describe your organization or you as a stakeholder (if applic… = Health research funding agency (includes foundations that fund health research (e.g., Health Research BC))
Q7 Please select the type of health research funding agency (if applicable) (select all that apply):
□ Not for profit
□ Charity
□ Government
□ Industry
□ Other _______________________________________________
Display this question:
Please select the term(s) that best describe your organization or you as a stakeholder (if applic… = Research organization
Q8 Please select the type of research organization (if applicable) (select all that apply):
□ University
□ University-affiliated research institute
□ Government
□ Non-governmental organization
□ Other _______________________________________________
Display this question:
Please select the term(s) that best describe your organization or you as a stakeholder (if applic… = Research user (e.g., member of the public or patient, government employee, journal staff, and healthcare provider)
Q9 Please select the type of research user (if applicable) (select all that apply):
□ Government employee
□ Journal staff
□ Clinician/healthcare provider
□ Health care manager
□ Member of the public or patient
□ Other _______________________________________________
Q10 The next several pages provide the recommendations organized by the four themes from the World Health Organization’s health research systems framework (governance/stewardship, financing, capacity building, and producing and using research). There are 12 recommendations, each of which is followed by a number of specific examples on how these recommendations could be implemented. Please select the example that represents your highest priority as an implementation focus for each of the 12 recommendations. Next, please indicate who should be responsible for implementing it such as Health Canada, the Canadian Institute of Health Research (CIHR), the provincial/territorial governments, universities, research institutes, etc. Note that you can click on the hyperlinked terms in some of the statements to obtain definitions/more information.
Q11 Theme 1: governance/stewardship
Q12 Recommendation 1: Outline research logistics as a part of emergency preparedness.
Please select your prioritized example for implementing the above recommendation from the following list:
◯ a. Create an emergency preparedness research plan that includes data sharing (across provinces/territories and national partners), cybersecurity, research ethics boards (REB) approvals, protocols for key studies on health emergencies that are pre-cleared by REB, and supply chain procedures.
◯ b. Develop an emergency preparedness plan that coordinates research questions with international research funders to prioritize based on capacity, expertise, infrastructure, and ensure the emergency preparedness plan is fully integrated with existing research policies.
◯ c. Centralize, standardize, and harmonize REB processes nationally with a single online form and centralized intake with reviews distributed to regional REBs according to their wait times, standardized training, and tracking of timelines.
◯ d. Prioritize REB for relevant studies during health/public health emergencies, maintaining an equity focus in the research.
◯ e. Harmonize processes (including data collection, privacy, REB, and searchable database) for biobanks (a repository of biological samples that are used in research) and data sharing (the dissemination and exchange of data/research findings for the purpose of further research) within provinces/territories and across provinces/territories to facilitate rapid research.
Q13 Who do you think should implement your prioritized example? (select all that apply)
□ Health Canada
□ Public Health Agency Of Canada (PHAC)
□ Canadian Institutes of Health Research (CIHR)
□ Provincial/territorial governments
□ Research institutes
□ Provincial/territorial funding agencies
□ Universities
□ Research charities
□ Patients/public
□ Health care professional organizations
□ Other_______________________________________________
Q14 Please provide any comments or suggestions for the above recommendation:
Q15 Recommendation 2: Prioritize equity and inclusion in research processes.
Please select your prioritized example for implementing the above recommendation from the following list:
◯ a. Use equity and anti-oppression principles in all governance decision making and actions aligned with the Tri-Council Agency’s Dimensions Charter and the rights of First Nations, Inuit, and Métis Peoples.
◯ b. Include patients/public at all governance levels in the health research ecosystem using an open, transparent recruitment process and publicly report on their inclusion.
◯ c. Create national database of ongoing studies for patients to engage with as research partners and research leads.
Q16 Who do you think should implement your prioritized example? (select all that apply)
□ Health Canada
□ Public Health Agency Of Canada (PHAC)
□ Canadian Institutes of Health Research (CIHR)
□ Provincial/territorial governments
□ Research institutes
□ Provincial/territorial funding agencies
□ Universities
□ Research charities
□ Patients/public
□ Health care professional organizations
□ Other_______________________________________________
Q17 Please provide any comments or suggestions for the above recommendation:
Q18 Recommendation 3: Facilitate streamlined, inclusive, and rigorous application and grant review process.
Please select your prioritized example for implementing the above recommendation from the following list:
◯ a. Monitor grant application and success rates by applicants’ PROGRESS PLUS factors (an acronym used to identify characteristics that stratify health opportunities and outcomes) and sex- and gender-based analysis plus (GBA+), report on this information publicly, and use it to inform and revise grant competitions (e.g., prioritize specific research areas, researchers who are experiencing structural barriers, etc).
◯ b. Ensure equity and diversity principles are embedded within all requests for proposals and grant applications, including the consideration that research team and patient partners should reflect the diversity of relevant population and that study team and participant demographics are reported to granting agencies to ensure they are reflective of population.
◯ c. Reimburse peer reviewers for any caregiving support required for their dependents, to enable the peer reviewers to attend meetings (e.g., implemented at Canadian Institute of Health Research (CIHR)).
◯ d. Ensure peer reviewers are trained in anti-oppression in research, equity, and diversity principles.
◯ e. Mandate that principal investigators with peer-reviewed grants must participate in grant peer review for the duration of their grant support.
◯ f. Standardize virtual and hybrid processes for grant peer review.
◯ g. Include patients in grant peer review process.
◯ h. Use Public Health Agency of Canada’s Strengthening the Integration of Intersectionality Theory in Health Inequality Checklist when reviewing grants to assess if and how research applicants adhere to equity considerations.
◯ i. Create multidisciplinary (e.g., Canadian Institutes of Health Research (CIHR) pillars 1 to 4) grant review panels and provide peer review training for multidisciplinary research.
◯ j. Create iterative grant peer review process with opportunity for interviews with applicants and peer review panel to clarify questions/responses.
◯ k. Streamline the grants application process for patients such as reducing requirements for patients to complete letters of support, CVs, and sex- and gender-based analysis plus (GBA+) modules, include patient-friendly instructions and modules.
◯ l. Conduct peer review of the grant peer review process (including peer reviewers) and make results of this peer review transparent.
◯ m. Ensure patients are adequately compensated to ensure they have capacity to participate as peer reviewers
Q19 Who do you think should implement your prioritized example? (select all that apply)
□ Health Canada
□ Public Health Agency Of Canada (PHAC)
□ Canadian Institutes of Health Research (CIHR)
□ Provincial/territorial governments
□ Research institutes
□ Provincial/territorial funding agencies
□ Universities
□ Research charities
□ Patients/public
□ Health care professional organizations
□ Other_______________________________________________
Q20 Please provide any comments or suggestions for the above recommendation:
Q21 Recommendation 4: Create communications infrastructure.
Please select your prioritized example for implementing the above recommendation from the following list:
◯ a. Develop centralized processes to communicate and coordinate research priorities with knowledge users (such as researchers, academic institutions, charitable organizations, and patient/public organizations including equity-deserving groups).
◯ b. Develop protocols and processes for rapid funding calls (e.g., ensuring they include focus on populations that may be at highest risk of health inequities).
◯ c. Encourage the use of communication platforms between Tri-Council Agencies and international funding agencies to facilitate alignment of research priorities in pandemics/health emergencies to coordinate communication around research (e.g., Global Research Collaboration for Infectious Disease Preparedness (GloPID-R)).
◯ d. Develop principles of transparent communication around what research is funded, including publicly reporting data on research impact and overall impact of research funding.
Q22 Who do you think should implement your prioritized example? (select all that apply)
□ Health Canada
□ Public Health Agency Of Canada (PHAC)
□ Canadian Institutes of Health Research (CIHR)
□ Provincial/territorial governments
□ Research institutes
□ Provincial/territorial funding agencies
□ Universities
□ Research charities
□ Patients/public
□ Health care professional organizations
□ Other_______________________________________________
Q23 Please provide any comments or suggestions for the above recommendation:
Q24 Recommendation 5: Coordinate research efforts across local, provincial, national, and international entities.
Please select your prioritized example for implementing the above recommendation from the following list:
◯ a. Leverage and extend the use of the Canada Research Coordinating Committee (CRCC) across the Tri-Council Agencies and the Canada Foundation for Innovation (CFI) to provide research and innovation advice, oversight, democratic decision-making, and coordination, prioritization, and communication across the Tri-Council Agencies and among international funding agencies.
➢ Membership of the CRCC should include national (e.g., Canadian Institutes of health Research (CIHR), Health Canada, Public Health Agency of Canada (PHAC)) and provincial/territorial funding agencies (e.g., National Alliance of Provincial Health Research Organisations (NAPHRO)).
➢ This could be achieved, for example, through strategies to create better coordination, as suggested in the recent report of the Advisory Panel on the Federal Research Support System. This report suggested creating a new entity, entitled the Canadian Knowledge and Science Foundation (CKSF) to rapidly address emerging research and innovation needs, deliver Tri-Council Agency programming, and enhance coordination, planning, and policy capacity across the research support system.
◯ b. Establish a health research funding agency in each province/territory where these do not currently exist and through which the provincial/territorial health ministry and public health agency can connect on research priorities and evidence needs.
Q25 Who do you think should implement your prioritized example? (select all that apply)
□ Health Canada
□ Public Health Agency Of Canada (PHAC)
□ Canadian Institutes of Health Research (CIHR)
□ Provincial/territorial governments
□ Research institutes
□ Provincial/territorial funding agencies
□ Universities
□ Research charities
□ Patients/public
□ Health care professional organizations
□ Other_______________________________________________
Q26 Please provide any comments or suggestions for the above recommendation:
Q27 Theme 2: financing
Q28 Recommendation 6: reimagine funding of research.
Please select your prioritized example for implementing the above recommendation from the following list:
◯ a. Embed equity considerations in decision making on all research investments, such as making funding contingent on meaningful actions to address inequities.
◯ b. Ensure long-term funding for successful research enterprises and develop strategies that balance defunding low impact initiatives and exploratory research.
◯ c. Assess extent to which research infrastructure and research infrastructure funding exists for therapeutics, vaccine, diagnostic testing development and implementation and develop metrics for appropriate allocation.
◯ d. Establish funding and sustainability strategies for provincial/territorial health research hubs with linkages to health, public health, social care, education, and cross-disciplinary collaborations (e.g., National Institute for Health and Care Research (NIHR) Clinical Research Networks, Applied Research Collaborations, National Health and Medical Research Council (NHMRC) Translational Research Centres, and National Institutes of Health (NIH) Implementation/translation Research Centres).
◯ e. Increase overhead/indirect cost allowance (cost of doing research including space, human resources, and contracts support) for research institutes to 50% to completely cover cost of research operations.
◯ f. Engage with industry to transparently contribute to funding and communications for health research authorities/hubs/networks/platforms.
◯ g. Work with industry to provide unrestricted funds for project research grants and infrastructure grants, with transparency protocols.
◯ h. Ensure separate funding for knowledge user-driven and researcher-driven research.
◯ i. Support mechanisms for crowdfunding research.
◯ j. Provide more support for researcher success (e.g., increase funding pool and/or support increased application quality).
◯ k. Increase access for non-academic organizations (e.g., local health authorities) to research funding pools.
◯ l. Include funding requirements and fund access to support patient involvement as research partners (e.g., honoraria, translation, and childcare), while considering patients’ circumstances (e.g., disability income and tax implications).
Q29 Who do you think should implement your prioritized example? (select all that apply)
□ Health Canada
□ Public Health Agency Of Canada (PHAC)
□ Canadian Institutes of Health Research (CIHR)
□ Provincial/territorial governments
□ Research institutes
□ Provincial/territorial funding agencies
□ Universities
□ Research charities
□ Patients/public
□ Health care professional organizations
□ Other_______________________________________________
Q30 Please provide any comments or suggestions for the above recommendation:
Q31 Theme 3: capacity building
Q32 Recommendation 7: Invest in formative training opportunities rooted in equity, diversity, and anti-racism.
Please select your prioritized example for implementing the above recommendation from the following list:
◯ a. Embed formative equity, diversity, and anti-racism components in all research capacity building activities.
◯ b. Provide training for researchers on trauma-informed approaches to patient engagement; that is, approaches rooted in an understanding of how trauma impacts people, with the purpose of avoiding potential re-traumatization during the research process. These approaches also acknowledge broader social contexts and how systems of oppression (e.g., colonialism and white supremacy) cause trauma.
◯ c. Provide training for researchers, patient partners, and policy-makers on anti-oppression practices in research; that is, practices that name and seek to dismantle injustices and power imbalances in the broader social context and in the research processes (e.g., asking community members most impacted by the research to lead key research activities such as developing the project plan and the budget).
◯ d. Provide training for researchers, patients, and policy-makers on patient engagement and knowledge mobilization.
◯ e. Establish a national standard for engaging patients as partners in research.
Q33 Who do you think should implement your prioritized example? (select all that apply)
□ Health Canada
□ Public Health Agency Of Canada (PHAC)
□ Canadian Institutes of Health Research (CIHR)
□ Provincial/territorial governments
□ Research institutes
□ Provincial/territorial funding agencies
□ Universities
□ Research charities
□ Patients/public
□ Health care professional organizations
□ Other_______________________________________________
Q34 Please provide any comments or suggestions for the above recommendation:
Q35 Recommendation 8: support researchers.
Please select your prioritized example for implementing the above recommendation from the following list:
◯ a. Create support strategies for those disproportionately affected systematically and during the pandemic such as Black, Indigenous, and people of colour, women, non-binary people, and clinician scientists.
◯ b. Use provincial/territorial/national data to estimate needs for the health human workforce and the research workforce using dynamic modelling (e.g., align training opportunities while monitoring for burnout/lack of retention).
◯ c. Create salary support pathways for scientists/clinician scientists (such as salary support awards or embedding salary into grants) throughout their career trajectories from early career to mid- and senior-career.
◯ d. Provide sufficient funding for researchers for knowledge mobilization, including in communication, media, and graphic design.
Q36 Who do you think should implement your prioritized example? (select all that apply)
□ Health Canada
□ Public Health Agency Of Canada (PHAC)
□ Canadian Institutes of Health Research (CIHR)
□ Provincial/territorial governments
□ Research institutes
□ Provincial/territorial funding agencies
□ Universities
□ Research charities
□ Patients/public
□ Health care professional organizations
□ Other_______________________________________________
Q37 Please provide any comments or suggestions for the above recommendation:
Q38 Recommendation 9: Support early career researchers.
Please select your prioritized example for implementing the above recommendation from the following list:
◯ a. Create opportunities for Postdoctoral Fellows to work in more than 1 sector (academic, industry, or government) during a fellowship.
◯ b. Create transdisciplinary research training networks for graduate students, fellows, and early career researchers to facilitate research and research training in diverse methods and disciplines across all research pillars (e.g., implementation science, One Health, artificial intelligence (AI)).
Q39 Who do you think should implement your prioritized example? (select all that apply)
□ Health Canada
□ Public Health Agency Of Canada (PHAC)
□ Canadian Institutes of Health Research (CIHR)
□ Provincial/territorial governments
□ Research institutes
□ Provincial/territorial funding agencies
□ Universities
□ Research charities
□ Patients/public
□ Health care professional organizations
□ Other_______________________________________________
Q40 Please provide any comments or suggestions for the above recommendation:
Q41 Theme 4: producing and using research
Q42 Recommendation 10: further strengthen Indigenous health research and break down systemic barriers to its conduct.
Please select your prioritized example for implementing the above recommendation from the following list:
◯ a. Sustain Indigenous-led biobanks and data sharing.
◯ b. Incorporate guidance and knowledge to support respectful research engagement with Indigenous people including the OCAP Principles (Ownership, Control, Access, and Possession), the OCAS principles (Ownership, Control, Access, and Stewardship) and Inuit Qaujimajatuqangit (Inuit traditional knowledge).
◯ c. Ensure barriers are removed for Indigenous knowledge holders to be principal applicants.
Q43 Who do you think should implement your prioritized example? (select all that apply)
□ Health Canada
□ Public Health Agency Of Canada (PHAC)
□ Canadian Institutes of Health Research (CIHR)
□ Provincial/territorial governments
□ Research institutes
□ Provincial/territorial funding agencies
□ Universities
□ Research charities
□ Patients/public
□ Health care professional organizations
□ Other_______________________________________________
Q44 Please provide any comments or suggestions for the above recommendation:
Q45 Recommendation 11: Produce innovative research.
Please select your prioritized example for implementing the above recommendation from the following list:
◯ a. Create partnership grants between researchers and knowledge users to focus on research uptake.
◯ b. Further develop multidisciplinary, collaborative grants across the Tri-Council Agencies (leveraging New Frontiers in Research Fund) that support collaborations across research disciplines including those that range from developing the team/research project through to completion of research and its dissemination.
◯ c. Create health research hubs within provinces/territories to link health care delivery context with research across all Canadian Institutes of Health Research (CIHR) pillars; include patient/public engagement and commercialization and facilitate a national network of these hubs (e.g., UK National Institute for Health and Care Research (NIHR) Applied Research Collaborations, National Health and Medical Research Council (NHMRC) Translational Research Centres).
◯ d. Embed clinical trials platform(s) within health care delivery/health research hubs (e.g., National Institute for Health and Care Research (NIHR)).
◯ e. Have funding calls for research areas prioritized by patients/the public.
Q46 Who do you think should implement your prioritized example? (select all that apply)
□ Health Canada
□ Public Health Agency Of Canada (PHAC)
□ Canadian Institutes of Health Research (CIHR)
□ Provincial/territorial governments
□ Research institutes
□ Provincial/territorial funding agencies
□ Universities
□ Research charities
□ Patients/public
□ Health care professional organizations
□ Other_______________________________________________
Q47 Please provide any comments or suggestions for the above recommendation:
Q48 Recommendation 12: enhance research use across the health research ecosystem.
Please select your prioritized example for implementing the above recommendation from the following list:
◯ a. Enhance science to policy dissemination training for researchers (e.g., in plain language communication) and policy-makers through various approaches including modules and embedded training opportunities.
◯ b. Create a network of chief science advisors in each national/provincial/territorial government department. Create opportunities for these advisors via knowledge exchange with researchers across Canada. These advisors can interpret and communicate science to policy-makers including communication of evidence uncertainty.
◯ c. Create knowledge exchange opportunities across funded networks/platforms/hubs.
◯ d. Co-create and deliver public education strategies for increasing health research literacy with members of the public.
◯ e. Co-create and deliver training for patients on engaging in research.
◯ f. Co-create and deliver training for patients on interacting with policy-makers.
Q49 Who do you think should implement your prioritized example? (select all that apply).
□ Health Canada
□ Public Health Agency Of Canada (PHAC)
□ Canadian Institutes of Health Research (CIHR)
□ Provincial/territorial governments
□ Research institutes
□ Provincial/territorial funding agencies
□ Universities
□ Research charities
□ Patients/public
□ Health care professional organizations
□ Other_______________________________________________
Q50 Please provide any comments or suggestions for the above recommendation:
Information & Authors
Information
Published In

FACETS
Volume 9 • Number 1 • January 2024
Pages: 1 - 44
Editor: Russel MacDonald
History
Received: 14 December 2023
Accepted: 19 April 2024
Version of record online: 6 September 2024
Notes
This paper is part of the Royal Society of Canada's COVID-19 Task Force Collection.
Copyright
© 2024 The Author(s). This work is licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Data Availability Statement
Data generated or analyzed during this study are not available due to the nature of this research. Specifically, according to the Research Ethics Board (REB) protocol approved for this study, only the research team members have direct access to the primary (raw) data, which will remain in password-protected files on hospital administrative servers/drives.
Key Words
Sections
Subjects
Plain Language Summary
Building a Better Health Research System in Canada: Insights and Actions from the COVID-19 Pandemic
Authors
Author Contributions
Conceptualization: SES, TC, BH
Data curation: RB, NP
Formal analysis: RB, NP, DK
Funding acquisition: SES, TC, BH
Investigation: SES, RB, CF, NP, DK, TC, BH
Methodology: SES, RB, CF, NP, DK
Project administration: RB, NP
Resources: SES, CF, DK, TC, BH
Software: DK, RB, NP
Supervision: SES, CF, DK, TC, BH
Validation: CF, DK, SES
Visualization: SES, TC, BH
Writing – original draft: SES, RB, NP, DK, TC, BH
Writing – review & editing: SES, RB, CF, NP, DK, TC, BH
Competing Interests
Tammy Clifford is the Vice-President of Research Programs at the CIHR and Bev Holmes is the president and CEO of Health Research BC. The remaining authors have declared that no conflicts of interest exist.
Funding Information
This work was funded by the Royal Society of Canada and the Canadian Institutes of Health Research (CIHR). The knowledge exchange sessions and surveys were conducted in partnership with the Royal Society of Canada and the CIHR.
Metrics & Citations
Metrics
Other Metrics
Citations
Cite As
Sharon E. Straus, Robyn Beckett, Christine Fahim, Negin Pak, Danielle Kasperavicius, Tammy Clifford, and Bev Holmes. 2024. Royal Society of Canada working group on health research system recovery: strengthening Canada’s health research system after the COVID-19 pandemic. FACETS.
9: 1-44.
https://doi.org/10.1139/facets-2023-0233
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
There are no citations for this item