Bat handlers, bat bites, and rabies: vaccination and serological testing of humans at risk
Publication: FACETS
8 November 2024
Abstract
Globally, bats provide critical ecosystem services. Rabies, caused by rabies virus and related lyssaviruses, is one of the most significant zoonoses associated with bats. Bat biologists study bats in the laboratory and the field. To minimize the risk of disease, all bat handlers should be vaccinated against rabies and undergo routine serological testing to measure their rabies virus neutralizing antibody levels. They should use best practices to avoid exposures, such as personal protective equipment, especially gloves appropriate to the size of the bat(s) being handled. Attention to such details will prevent unnecessary exposures and avoid some of the accompanying negative perceptions that endanger bats on a global level. The small body sizes of many bats (<50 g, many <20 g) and small teeth makes their defensive bites easy to overlook. Breaks in the skin, however small, may result in exposure to lyssaviruses in the animals’ saliva. Exposure to blood-feeding bats is less common because these species are geographically restricted to the Neotropics and are the only species whose natural feeding behavior could involve transmission of rabies virus. Understanding viral transmission, preventing exposures, and responding appropriately to bites will minimize the consequences of this deadly zoonosis.
Introduction
The mammalian order Chiroptera is composed of ∼1500 species of extant bats (Simmons and Cirranello 2024). Bats are the only mammals capable of powered flight. The highest diversity of bats occurs in the tropics and subtropics. Wherever they occur, bats play critical roles in ecosystem services although these are often most apparent when populations decline (e.g., Frank 2024). Bats are fascinating animals and researchers the world over study them in the laboratory and field. Their attraction as subjects is longstanding as reflected by the many books about bats published over the past century (e.g., Allen 1939; Griffin 1958; Brosset 1966; Kunz and Parsons 2009; Fenton and Simmons 2015; Fenton and Rydell 2023). Human health risks associated with the study of bats and other wildlife can be mitigated by precautions around exposure to zoonotic viruses such as rabies lyssavirus (RABV) (Messenger et al. 2003).
Multiple lyssaviruses cause rabies (Table 1), a major viral zoonosis that can spill over to humans from other animals including humans (Warren and Sawyer 2023). This is an acute progressive neurological disease of mammals which, following the onset of illness, is almost invariably fatal because there is no proven treatment for it in any species. The clinical disease rabies is caused predominantly by RABV, a single-stranded, negative-sense, RNA virus in the family Rhabdoviridae (Kuhn et al. 2022). Rabies also is caused by at least 17 other putatitve lyssavirus species (Coertse et al. 2020), including Kotalahti bat lyssavirus which awaits formal classification, as well as Matlo bat lyssavirus, Taiwan bat lyssavirus 2, and Phala bat lyssavirus (Walker et al. 2022). In afflicted animal vectors, lyssaviruses are excreted in saliva. Bites are the main route of viral transmission. Besides bites or scratches, conspecific grooming and licks to open wounds may result in exposure from animals with high amounts of salivary viral shedding (Banyard et al. 2020; Gregory and Tinline 2020). Conventionally mucous membrane exposure involves recipient ocular, oral, rectal, or vaginal exposures.
Table 1.
| Recognized species | Common name | Phylogroup* | Distribution |
|---|---|---|---|
| Lyssavirus aravan | Aravan virus (ARAV) | I | Eurasia |
| Lyssavirus australis | Australian bat lyssavirus (ABLV) | I | Australia |
| Lyssavirus bokeloh | Bokeloh bat lyssavirus (BBLV) | I | Europe |
| Lyssavirus duvenhage | Duvenhage virus (DUVV) | I | Africa |
| Lyssavirus hamburg | European bat lyssavirus 1 (EBLV-1) | I | Europe |
| Lyssavirus helsinki | European bat lyssavirus 2 (EBLV-2) | I | Europe |
| Lyssavirus gannoruwa | Gannoruwa bat lyssavirus (GBLV) | I | Sri Lanka |
| Lyssavirus ikoma | Ikoma virus (IKOV) | III | Africa |
| Lyssavirus irkut | Irkut Virus (IKRV) | I | Eurasia |
| Lyssavirus khujand | Khujand virus (KHUV) | I | Eurasia |
| Lyssavirus lagos | Lagos bat virus (LBV) | II | Africa |
| Lyssavirus lleida | Lleida bat virus (LLEBV) | III | Western Europe |
| Lyssavirus mokola | Mokola virus (MOKV) | II | Africa |
| Lyssavirus rabies | Rabies virus (RABV) | I | Global† |
| Lyssavirus shimoni | Shimoni bat virus (SHIBV) | II | Africa |
| Lyssavirus formosa | Taiwan bat lyssavirus (TWBLV) | I | Asia |
| Lyssavirus caucasicus | West Caucasian bat virus (WCBV) | III | Eurasia |
Note: Distributions are approximate.
*
Note: Common licenced vaccines lack cross-reactivity with lyssaviruses in phylogroups II and III.
†
With a few exceptions.
Globally, rabies is responsible for tens of thousands of human deaths annually. The numbers of human fatalities vary among countries. Unfortunately, surveillance for RABV and other lyssaviruses is poor in several regions such as in many low- to middle-income countries (LMICs) (Stockstad 2017; Barbosa et al. 2018; Castillo-Neyra et al. 2020; Gan et al. 2023). Most human fatalities from rabies occur in Asia and Africa. Globally, dog rabies poses the greatest threat to humans as dogs are a commonly infected reservoir of RABV and are in close contact with people. Indeed, rabid dogs cause >99% of all human deaths from rabies (Taylor et al. 2017). Mass vaccinations have reduced the incidence of rabies in dogs in many parts of the world but not everywhere (Fahrion et al. 2023). In North America, human deaths from rabies have decreased dramatically since 1960 because of rabies prevention and control in dogs. Most North American cases now result from interactions with wildlife—mainly bats (Pieracci et al. 2019; Fenton et al. 2020a, 2020b; Ma et al. 2023). The “Zero by 30” program proposed by the Food and Agriculture Organization of the United Nations, World Organization for Animal Health (WOAH), and World Health Organization (WHO) has focused on global elimination of human cases from rabid dogs by 2030, but deaths from rabies caused by other animals, including wildlife, will continue.
Bats are important reservoirs of lyssaviruses, but, in contrast to many other mammals, are typically small-bodied animals. Compared to a bite from a dog, cat, or other carnivore, a bat bite is much less spectacular and often not as easily recognized (Fig. 1). Even a bite from a small (<10 g) bat infected with RABV can be fatal when the teeth penetrate the skin (Kunkel et al. 2022). When a bat bites, the resulting lesion may bleed, but not always. A bite site may be difficult for a person to detect, even shortly after the bite (Jackson and Fenton 2001; Fenton et al. 2020a, 2020b). This means that neither the patient nor healthcare personnel may be able to find evidence of a bat bite in all cases (Fig. 1). If the biting bat has been captured, then its brain can be tested for evidence of a lyssavirus infection. In some areas testing is not readily available or may be delayed. Public health personnel should undertake a thorough risk assessment and consider postexposure prophylaxis (PEP) to exposed individuals. If the bat that bit is not available, public health personnel should undertake a thorough risk assessment and consider PEP to exposed individuals. This protocol includes wound care, specifically injection of rabies immune globulin (RIG) into and around the wound in unvaccinated persons and a series of rabies vaccinations. In many parts of the world, surveillance for rabies is uncommon as is rapid and appropriate PEP.
Fig. 1.

The purpose of this perspective is to provide information about rabies vaccinations and the immunity they can confer for individuals at risk of viral exposure. We emphasize these issues to field biologists and technical personnel who work with bats and/or rehabilitate them. As bats are nocturnal, cryptic, and the world’s only flying mammals, they are often the focus of myths, negative associations, and misconceptions (Fenton and Simmons 2015; Fenton et al. 2020a, 2020b). Additionally, the public perception of the risks associated with bats is strongly influenced by the fact that some species are reservoirs of lyssaviruses (Fenton and Rydell 2023; Fenton et al. 2020c). Importantly, bats showing clinical signs of rabies do not recover from the infection and do not chronically excrete virus (Moreno and Baer 1980; Franka et al. 2008). Rabies is an acute infectious disease that kills bats as well as other mammals (Moreno and Baer 1980; Franka et al. 2008). Even so, bats have an astonishing resistance to many viral infections, including the capacity to frequently clear lyssaviruses before a productive infection establishes (Blackwood et al. 2013). This has spurred renewed interest in studying bat immunity (Blackwood et al. 2013; Irving et al. 2021; Banerjee and Mossman 2022).
Vaccines and titres
Taxonomically, lyssaviruses may be divided into different phylogenetic groups. There are effective vaccines against RABV and other phylogroup I lyssaviruses, but not against phylogroups II and III and the unassigned viruses (WHO 2017). Current preexposure prophylaxis (PrEP) consists of vaccinations and booster schedules for persons in different exposure risk categories. The specific PrEP vaccination recommendations vary with locality (e.g., United Kingdom: see Brown and Russell 2020; United States: see Rao et al. 2022). In contrast, PEP includes both vaccine and RIG administration to unvaccinated persons.
Operationally, vaccination against RABV is a two-step process. Both steps must be completed before anyone has the immunity necessary to work with bats or other rabies vector species.
Step one is PrEP vaccinations, which provide immunization against RABV. Persons who work with wild mammals or RABV in the laboratory should always receive PrEP. Step two is testing the level of rabies virus neutralizing antibody (RVNA) present in the patient’s serum (serology test). To be clear, neither the Advisory Committee on Immunization Practices (ACIP) nor the WHO recommend a RVNA titre check after routine PrEP for most individuals such as travelers (WHO 2018; Rao et al. 2022). However, ACIP recommends RVNA checks based on risk levels. Moreover, WHO recognizes that the timing of serological monitoring is based on risk level and is decided by the worker’s supervisor/employer responsible for assessing the relative risk of viral exposure (Rao et al. 2022).
While neither ACIP nor WHO recommend RVNA titre check after routine PrEP for most individuals (Rao et al. 2022; WHO 2018), both recommend it for individuals at higher risk of exposure. It is our opinion that handling of bats during research puts researchers in a higher-risk category, and that step 2 is a key component of working safely with bats.
As noted above, both steps should be completed before people begin working with bats or other mammals of concern, such as mesocarnivores (e.g., coyotes, dogs, foxes, mongooses, raccoons, skunks, and jackals). After PrEP, it is important to carry proof of vaccinations and RVNA titre checks. Ideally, workers should have regular tests of their RVNA (i.e., a titre at least every two years). The suggested frequency of serological surveillance will vary based on risk level (Rao et al. 2022). Note that neither PrEP nor RVNA testing is available everywhere. Bat biologists and other handlers at high risk of viral exposure should complete both steps before traveling to a field or laboratory site where there is a risk of exposure to RABV or other lyssaviruses. Specific requirements and recommendations vary geographically.
The WHO recommends rabies vaccination with cell-culture derived viruses or embryonated egg-based rabies vaccines (WHO 2018). Even though rabies is almost invariably fatal after symptoms appear, death is also almost always preventable when PEP is administered in a timely and appropriate manner (Jackson and Fenton 2001). In some countries, besides intramuscular (IM) vaccine administration, intradermal (ID) administration with 0.1 mL of vaccine is also recommended by the WHO to conserve vaccine (Brown and Russell 2020). In general, a serological value of ≥0.5 IU/mL is the recommended RVNA titre for an adequate response to vaccination against RABV (and presumably against related lyssaviruses in phylogroup I).
Testing RVNA levels based on risk is important because, although uncommon, not everyone develops a titre of ≥0.5 IU/mL after receiving a course of PrEP vaccinations. For example, in a survey of 280 patients (Mansfield et al. 2016), some were considered “good responders” because they maintained a RVNA of ≥0.5 IU/mL even 10 years after their initial vaccination. Others were “poor responders” because they did not maintain adequate RVNA levels after one year. A two-dose PrEP series is now endorsed by both the ACIP and WHO, but local recommendations may vary. In a study of multiple treatment groups (i.e., three-dose and two-dose IM, three-dose and two-dose ID), the percentage of responders after one year with titres ≥0.5 IU/mL were 64%, 58%, 45%, and 60%, respectively (Endy et al. 2020). These results reinforce the observation of the “good” responder/poor responder dichotomy.
Information about rabies serology testing and where to send samples from both people and animals for testing in the USA and Canada can be found at these sites:
Working with bats and managing exposures
Gloves are essential personal protective equipment (PPE) for people handling bats. The choice of gloves depends upon the size and disposition of the bat. When handling bats hold them firmly to avoid being bitten and gently to avoid injuring them. Bats are often quick to bite in self-defense, such as while being handled immediately after capture. A major point is that a bite from a bat that is behaving normally does not necessarily mean an exposure to a lyssavirus. The bat may have been agitated and defending itself rather than showing clinical signs of encephalitic or “furious” rabies. If the bite was unsolicited (i.e., an unprovoked bat landed on and then bit someone), this should be considered abnormal behavior and a high-risk exposure to a potentially rabid animal. Importantly, even an apparently “normal” animal can have rabies and excrete virus in its saliva for over 10 days before showing any abnormal clinical signs.
There is a range of clinical presentations among bats with rabies both among individuals of the same species and different species. Other illnesses and injuries may cause signs that could be confused with rabies. This means that bats with rabies cannot always be reliably recognized. Wherever possible, the bat(s) involved in an apparent exposure of people to virus should be safely captured, killed humanely, and its brain sent to be tested for RABV or any other lyssaviruses.
Regardless of their PrEP vaccination status, anyone with a potential exposure to RABV (or another lyssavirus) through an animal bite, scratch, or lick, should wash the site thoroughly with soap and water for at least 15 min. If the eyes were exposed, they should be rinsed thoroughly. Immediately thereafter, the person should contact their health care provider and/or report the incident to their local public health authority to ensure that a medical risk assessment is carried out (Brass 1994). Potentially, those who had previously received PrEP and whose RVNA titre was ≥0.5 IU/mL may be at lower risk with respect to developing rabies than those who received PrEP. Regardless, the patient should receive medical advice as soon as possible after the exposure. In situations where people are regularly exposed to bats, in addition to having PrEP they should have access to and use a first aid kit and with potable water and liquid soap.
Considering the above points, there are some misunderstandings about the utility of knowing the RVNA titre at the time of exposure for persons with PrEP (Moore 2021). Regardless of the RVNA level in persons with PrEP, booster doses are usually required because the RVNA level is a reflection of one aspect of adaptive, humoral immunity, but cannot provide fulsome information on outcome. Moreover, RVNA levels decline over time (World Health Organization 2017). There are gaps in our knowledge about what is needed for absolute efficacy against lyssaviruses and cross reactivity is not conferred by current vaccines against all non-RABV lyssaviruses (Echevarria et al. 2019). Moreover, the nearly 100% risk of human mortality after showing symptoms of rabies is too high not to provide maximum enhancement of immune effectors upon exposure. Animal studies provide information (and are encouraging) but evidence of circulating RVNA is not a guarantee of survival. Each exposure is unique based on factors such as the site of infection, the infectious viral dose, wound severity, and standing host immunity, among others. Adherence to current guidance/recommendations will enable ideal management in exposed individuals.
Modern rabies prophylaxis is safe, effective, and predictable in mounting an acceptable immune response in most individuals. However, the ideal immune response to rabies vaccination will vary based on host factors such as age, genetics, nutrition, and immune suppression (Pancharoen et al. 2001). This explains, in part, the incidence and variation associated with inadequate antibody titres after PrEP rabies vaccination, as reported in one study of veterinary medical students (Banga et al. 2014).
Prophylaxis for unvaccinated persons
All individuals who have been bitten or scratched by a (potentially) rabid animal, should wash the wound site thoroughly with soap and water for at least 15 min. They should present immediately to a health care facility (i.e., contact their health care provider and/or report the incident to their local public health office) so they can receive PEP in a timely fashion (Brass 1994). Although the number of PEP vaccine doses may vary from three to five (or more), it typically involves four—one each on days 0, 3, 7, and 14. Specific guidelines for PEP vary geographically (e.g., United Kingdom: see Brown and Russell 2023). In addition to vaccination, exposed unvaccinated individuals should receive RIG, anti-RABV antibodies produced commercially from another vaccinated human (human rabies immune globulin (HRIG)) or other species such as a horse (equine rabies immune globulin (ERIG)) (Brass 1994). In some countries, for example China and India, alternatives to RIG include using monoclonal antibodies against RABV (Chen et al. 2024; Tambe et al. 2024). These pre-made RVNAs provide immediate defense (passive immunization) against RABV until the exposed person can begin producing their own RVNA (active immunization) in response to vaccination. Critically, RIG or monoclonal antibodies are only administered once at the beginning of PEP and are typically given to individuals with wounds classified as a category III exposure (i.e., bites, scratches, and/or mucosal exposure). During PEP, wounds should be infiltrated with 20 IU/kg for HRIG (or 40 IU/kg of ERIG). The HRIG should not be administered if 7 days have passed after the first vaccination to avoid inhibition of the vaccine response. When an exposed person is suspected to be immune compromised, one or more additional doses of vaccine may be recommended (World Health Organization 2017, 2018). Serological testing for RVNA levels provides an indication of an appropriate immune response.
Prophylaxis for persons previously vaccinated for rabies
People who regularly handle bats with ungloved hands may suffer repeated bites. Such handling is unwise behavior, even for people who study bats and have RVNA levels ≥ 0.5 IU/mL. People handling live bats should always wear gloves. The bottom line: individuals that work with bats should obtain PrEP, monitor antibody RVNA levels, and keep records of the dates of vaccinations and titre readings. They should receive two doses of rabies vaccine for PEP when potentially exposed. When/if RVNA levels fall to < 0.5 IU/mL, an appropriate booster dose of vaccine should be administered. The 2018 WHO position paper has guidance for persons with repeated exposures as can happen with bat handlers (World Health Organization 2018). For example, if an individual has a repeat viral exposure within three months of a previous exposure, and has already received complete PEP, only wound care is required. Neither vaccine nor RIG is recommended by WHO. For repeat exposures occurring more than three months after the last PEP, the schedule for previously immunized individuals should be followed and RIG is not indicated. This is based on the typical timeline of the RVNA response after a booster (i.e, a rapid peak with a slow decline).
There are obvious financial and logistical costs associated with vaccinations and checks of RVNA levels. Globally, most people die from rabies because they did not receive PEP. Routinely exposed persons should receive 2 or 3 IM/ID doses for PrEP and 3 or 4 IM or ID doses for PEP. According to the WHO, many persons exposed to RABV face extreme difficulties receiving PEP because of shortages in biologics and/or costs of care. In Canada and the USA, a vial of rabies vaccine may cost $500 USD or more, so in 2022, the total price of a full series of IM vaccinations varies but was estimated to be ∼US$1000 for PrEP and ∼US$1350 for PEP, not including RIG (Fenton and Rydell 2023). An estimate of the cost of a three-dose PrEP may vary between US$1100 and US$3500 (Moore 2021), considering additional expenditures for the clinical visit, administration costs, etc. The situation for payment varies among countries. For example, in Brazil and other parts of Latin America, prophylaxis is free and publicly available. Unfortunately, this is not the case everywhere. All too often, logistical barriers can make finding PEP challenging. For example, distance to health facilities in peri-urban areas was one of several barriers to seeking vaccination after canine RABV exposures (de Paula Silva et al. 2021).
The ID route of administration follows the same dosing schedule but uses a lower volume of rabies vaccine (0.1 mL) compared to the IM route (1.0 mL). Importantly, because multiple doses of vaccine can be drawn from the same vial, more people can be vaccinated against RABV using the ID route of administration. Indeed, ID vaccinations have been used in rabies-endemic countries for decades because of the lower per person cost, which allows more people to be effectively and safely vaccinated against rabies (Brown and Russell 2020). In many research situations, laboratory personnel receive ID vaccinations for PrEP, when approved, which may reflect budget considerations and other constraints.
To reduce the costs associated with vaccinations, the WHO promotes using ID vaccination as a dose-savings alternative to IM vaccination. The ID route of vaccination results in a comparable RVNA response against RABV (WHO 2018; PHAC 2015). In Canada, ID rabies vaccinations are endorsed by the National Advisory Committee on Immunization for PrEP, but not for PEP. In the USA, ID vaccination is not licensed and is considered off-label use.
In the context of rabies, are certain bats more “dangerous” than others?
All bats, like other mammals, are susceptible to lyssaviruses although not all bat species are reservoirs for such viruses. World-wide, the nearly 1500 bat species range in adult size from ∼2 g to ≥1.5 kg and precautions should always be taken as if any bat anywhere could have rabies. The small size (usually ≤20 g) of most bat species means their bites are usually not obvious and (dangerously) may go unnoticed. The same goes for scratches from small bats’ claws (Dato et al. 2016). Not all bites and scratches show readily detectable lesions and are easy to overlook (Fenton et al. 2020a, 2020b). In this situation, even when the bat is rabid, the risk of exposure could be low because viral transmission is unlikely when the skin barrier has not been broken. However, it is essential to follow advice about washing the site of the bite or scratch and seeking medical attention. Humans accustomed to handling bats report that bats will lick a handler’s skin apparently to obtain salt or moisture. Licking a previously existing open wound could also transfer virus. Like other wildlife, bats should be handled only by experienced, vaccinated personnel who are using PPE, such as appropriate gloves.
The upper canine teeth of most bats are pointed and the longest in the tooth-row. Most often, these are the teeth that deliver skin puncture bites (Fig. 1), which can be painful even when delivered by small bats. Typically, but not always, bat bites present as two puncture marks: one each from the left and right upper canine tooth. Vampire bat defensive bites are noteworthy exceptions. Here, both the upper incisor and canine teeth are triangular, blade-like, and make scalpel-like cuts (Fig. 1D) rather than puncture wounds (Fig. 1A). Paradoxically, vampire bat defensive bites are sometimes rather painless because their teeth are so sharp.
The three species of vampire bats are the only bats whose feeding behavior involves biting prey (most often birds and mammals) to obtain blood (food). Feeding bites are shallow scrapes (∼5 mm long, ∼5 mm deep) made by the upper incisor teeth. These bites typically occur on sleeping prey. Such “normal” behavior can, however, transmit RABV if excreted in the bat’s saliva. Hence, when sleeping outdoors in areas with common vampire bats, sleep under a protective mosquito net. Feeding bites by common vampire bats can transmit RABV to people (Stoner-Duncan et al. 2014; Junior et al. 2023). In South America, some human deaths from rabies that appear to involve bats may not be from vampire bats (PHAC 2015). For example, recently in Brazil, four fatal pediatric cases arose from children catching bats and keeping them as pets (Junior et al. 2023). Bites on the children’s upper lips and elbows suggest that they were petting and not just handling the bats.
If someone is bitten by a bat, it can be useful to know the species for epidemiological purposes. However, trying to catch the bat that bit someone is likely to result in more bites, and capture does not guarantee identification of the bat species. When a bat that delivered an unprovoked bite is caught, in some jurisdictions (but not all), it should be tested for RABV or other lyssaviruses by current WHO/WOAH recommendations. There are records of bats testing positive for RABV variants usually associated with another bat species. For example, in North America a similar variant of RABV usually associated with Lasionycteris noctivagans (silver-haired bats SHB-RABV) has been reported from other bat species such as Perimyotis subflavus (tricolored bats). Similarly, RABV variants from vampire bats have been associated with other species. Such knowledge is important to consider for virus spill-over because these variants of RABV have accounted for multiple human deaths from rabies (Fenton et al. 2020b; Ma et al. 2023).
To complicate the issue about bats and RABV—infections to humans, all species of lyssaviruses can cause the disease rabies (Fig. 2). While current rabies vaccines are highly effective, we know that common licensed rabies vaccines may not provide adequate protection because they lack cross-reactivity to lyssaviruses in phylogroups II and III (Table 1) (Coertse et al. 2020, 2023). For example, some bats indigenous to Africa and Eurasia harbor lyssaviruses not neutralized by antibodies from existing vaccines (National Advisory Committee on Immunization 2006). However, cross-reaction may be possible with very high antibody titres (Hanlon et al. 2005) Cross-reactivity is determined not only by viral neutralization (i.e., seroneutralization) but also includes other methods such as epitopic mapping, experimental infection, and field observations of failure in vaccinated animals (Markotter and Coertse 2018; Fooks et al. 2021). Although many species of bats have tested positive for lyssaviruses, the number of species reported to be rabid is relatively small compared to the total diversity of bats. Reservoirs have been identified among common bat species where there are adequate data. Typically, surveillance is skewed to areas where monitoring for rabies in biting animals is a routine public health activity (Baer 1991; Klug et al. 2011). However in most areas the surveillance is inadequate. Most bats are not rabid, but given surveillance biases and problems with bat identification, we have no evidence that one bat species is any more at risk for spreading lyssaviruses than another. We do not know the specific bat variants that commonly cause human rabies. There is a small number of spill-over cases reported in other species (i.e., other bat species, stone martens, sheep, domestic cats) (Fooks et al. 2021; Racey et al. 2013; Folly et al. 2021) but we do not know how bats may be involved here.
Fig. 2.
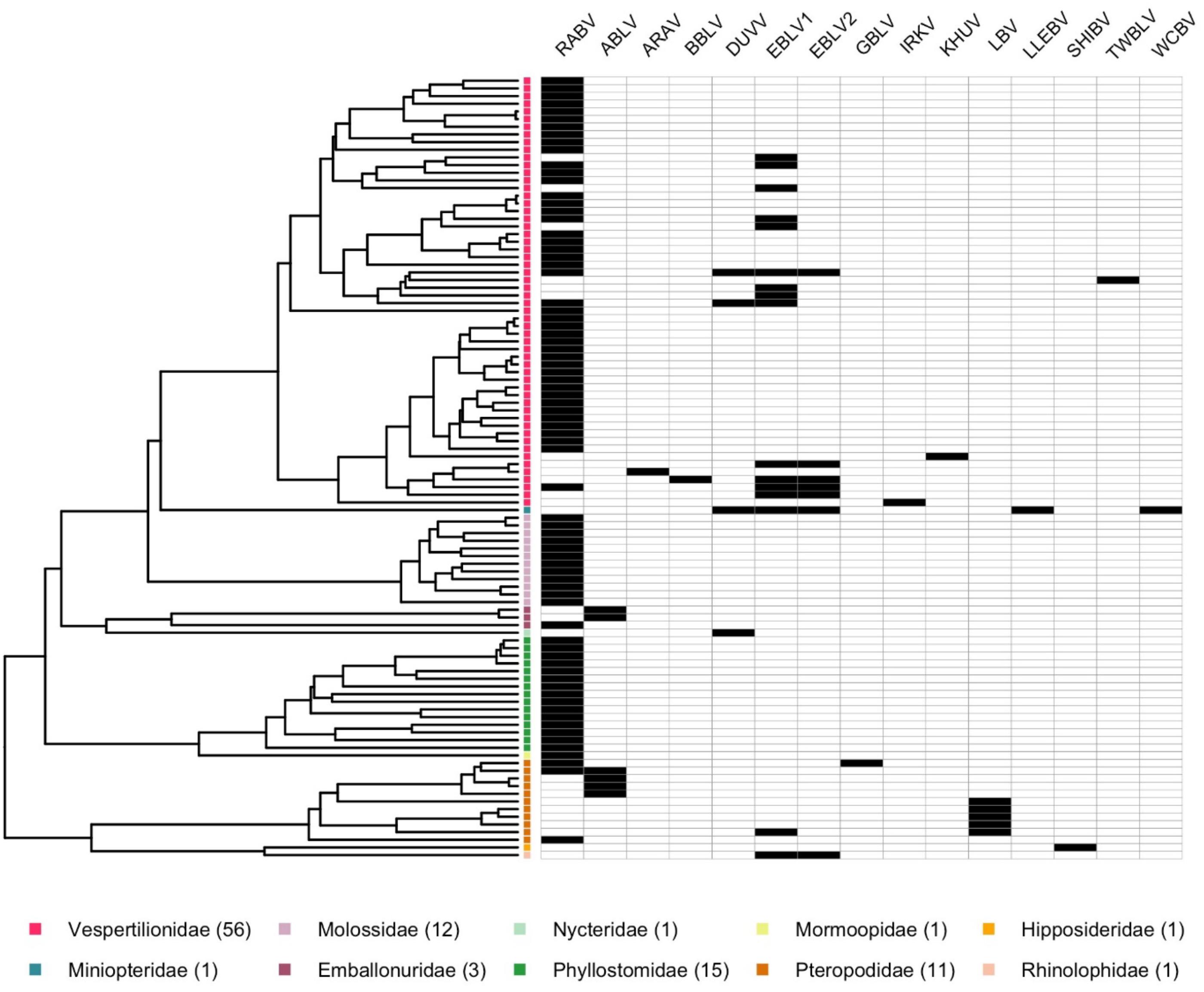
From a public health perspective, in the wild any bat could be rabid. Furthermore, bats in rehabilitation centres may show delay in onset of rabies. In the New World, spillover of RABV from bats often involves vampire bats, typically the common vampire bat, Desmodus rotundus (Fenton et al. 2020b). Common vampire bat RABV is closely related to RABV found in Brazilian free-tailed bats (Tadarida brasiliensis), and this variant is more closely related to North American than to South American Brazilian free-tailed bat RABV. Another RABV (variant 3 from South America) is more widespread. The other two species of vampire bats—the hairy-legged vampire (Diphylla ecaudata) and the white-winged vampire (Diaemus youngi)—although susceptible to RABV, have not yet been identified as competent reservoirs.
Notably, common vampire bat and Brazilian free-tailed bat RABV variants have spilled over and been recorded from several other bat species (Fenton et al. 2020b), including Carollia perspicillata (Seba’s short-tailed fruit bat), Diclidurus albus (northern ghost bat), Artibeus planirostris (flat-faced fruit-eating bat), and A. lituratus (great fruit-eating bat). This may be explained, in part, by roosting ecology because common vampire bats often roost with several other bat species. For example, at sites in Belize, they roost with Glossophaga soricina (Pallas’s long-tongued bat), Mimon cozumelae (Cozumelan golden bat), Carollia perspicillata (Seba’s short-tailed fruit bat), Saccopteryx bilineata (greater white lined bat), and Natalus mexicana (Mexican funnel-eared bat). Moreover, the presence of vampire bat RABV spillover into cats is yet another reason why humans should avoid bites from other mammals (Gan et al. 2023).
Rapid immunochromatographic test kits for rabies
When a person has been bitten by a bat or other suspected animal, rabies diagnostic tests recommended by WOAH and WHO would ideally be available within 24–48 h to determine the need for PEP, which, for maximum effectiveness in preventing death, should be administered as soon as possible. Laboratory-based surveillance is much less than ideal in many LMICs and even in some high income nations test results may not be available for many days. This presents a dilemma for wildlife biologists who have ready access to some testing and PEP not readily available to people living where they are doing field work. After any animal bite, immediate first aid entails washing the wound thoroughly with soap and water; however, medical advice, diagnostic testing, and modern biologics may otherwise not be readily available. In response to this situation, over the last several years, there have been advances in local point-of-care tests for rabies (Folly et al. 2021). These rapid immunochromatographic or lateral flow test kits have been used in resource-limited settings in Asia and Africa (Lechenne et al. 2016; Yale et al. 2019; Kimitsuki et al. 2020; Mauti et al. 2020; Tenzin et al. 2020; Fooks et al. 2021). Under the best conditions, sensitivity and specificity compare favorably to gold-standard rabies diagnostic tests. Basically, the suspect animal is killed humanely by recommended methods, its brain removed, a small sample of brain tissue is tested, and a visual result is obtained in a few minutes on a handheld lateral flow device similar to many home tests used for other pathogens (Tenzin et al. 2020). In the future, bat biologists and others may avail themselves of such point-of-care tests to help determine the status of a biting animal. However, decisions about PEP treatments should not be delayed or omitted on the basis of a negative test result. These tests may not be effective against all lyssaviruses (Klein et al. 2020).
Lyssaviruses
Historically, although rabies has been recognized for millennia, the ability to distinguish different viral species and variants occurred only by the late 20th century. To date, RABV is one of 17 virus species recognized by the International Committee on Taxonomy of Viruses (ICTV) as members of the genus Lyssavirus, with others awaiting classification (Table 1). Currently, RABV is the only lyssavirus found among bats in the New World (Fig. 2). By contrast, in the Old World, different lyssavirus species circulate in bats (Markotter and Coertse 2018; Mauti et al. 2020; Kimitsuki et al. 2020; Viljoen et al. 2023). Viral species definitions are generally based heavily on phylogenetics, but distribution in host species and other viral characteristics also are considered. The latest ICTV taxonomy is presented in Table 1. Divača bat lyssavirus is a more recently described variant (Černe et al. 2023) in phyllogroup I and associated with Myotis capaccinii in Slovenia.
Nine critical take home messages about rabies for bat biologists
1.
Do not handle bats with ungloved hands.
2.
Before working with bats, get PrEP and record RVNA level.
3.
For at least 15 min wash thoroughly all lesions from a bat bite or scratch, thoroughly with soap and water. This approach to treating dog bites has been highly effective in preventing rabies but does not eliminate the need for PEP.
4.
Remember, once a person shows clinical symptoms of rabies, it is virtually always fatal, so PEP should occur as soon as possible after a potential viral exposure. Even if a person with a potential RABV exposure is in a remote area, PEP often can still be successful if administered several days after the exposure. Moreover, if the person has had PrEP, they should still seek medical advice about boosters.
5.
Bats infected with lyssavirus may appear normal or show signs that may not be immediately associated with rabies.
6.
Bats are susceptible to RABV and other lyssaviruses. Any bat anywhere can be infected and die of rabies.
7.
Rabies, the disease, is caused by RABV and several other lyssaviruses. Every year in the Americas more people die from infections due to bat RABV than RABV from other wildlife (Fenton et al. 2020a; Pieracci et al. 2019). When working abroad, remember that laboratory-based surveillance for rabies in some LMICs may be suboptimal so it is important to be vigilant for a potential exposure.
8.
In the 21st century rabies is a vaccine-preventable disease and we understand its basic epidemiology and pathobiology. We have sensitive and specific diagnostics, as well as pure, potent, safe, effective, and affordable countermeasures to prevent rabies in humans.
9.
Any bite from a bat requires medical care. This brings us back to a fundamental question: how do bat biologists learn to handle bats and avoid bites that could infect them with a lethal virus? In addition to training students about how to catch and handle bats safely, training must provide background about rabies, the realities of the disease, the vaccinations that are available. the importance of PrEP and PEP and measures of (RVNA).
Acknowledgements
We thank all our colleagues in the bat and rabies fields for continuing to ensure that natural resources are used in a safe and productive manner according to global norms. We thank Professor Ryan Troyer for reading and commenting on an earlier version of the manuscript.
References
Allen G.M. 1939. Bats. Harvard University Press, Cambridge. 358p.
Baer G.M. 1991. The natural history of rabies. 2nd ed. CRC Press, Boca Raton. 1991. 620p.
Banerjee A., Mossman K. 2022. Laying the foundation for single-cell studies in bats. Immunity, 55: 1974–1977.
Banga N., Guss P., Banga A., Rosenman K.D. 2014. Incidence and variables associated with inadequate antibody titers after pre-exposure rabies vaccination among veterinary medical students. Vaccine, 32: 979–983.
Banyard A.C., Davis A.T., Gilbert A.T., Markotter W. 2020. Bat rabies. In Rabies. Edited by A.R. Fooks, A.C. Jackson. 4th ed. Elsevier Inc, San Diego. pp. 231–276.
Barbosa Costa G., Gilbert A., Monroe B., Blanton J., Ngam Ngam S., Recuenco S., Wallace R. 2018. The influence of poverty and rabies knowledge on healthcare seeking behaviors and dog ownership, Cameroon. PLoS One, 13(6): e0197330.
Blackwood J.C., Streicker D.G., Altizer S., Rohani P. 2013. Resolving the roles of immunity, pathogenesis, and immigration for rabies persistence in vampire bats. Proceedings of the National Academy of Sciences, 110: 20837–20842.
Brass D.A. 1994. Rabies in bats. Natural history and public health consequences. Livia Press, Ridgefield. 335p.
Brosset A. 1966. La biologie des Chiroptères. Masson et Cie, Paris. 231p.
Brown K., Russell K. 2023. Guidelines on managing rabies post-exposure (January 2023). Public Health England, UK Health Security Agency. Available from https://www.gov.uk/government/publications/rabies-post-exposure-prophylaxis-management-guidelines [accessed May 2024].
Brown K., Russell K. 2020. Guidelines on timing of rabies boosters based on antibody levels. Public Health England, UK Health Security Agency. Available from https://www.gov.uk/government/publications/rabies-post-exposure-treatment-timing-of-vaccine-booster/guidelines-on-timing-of-rabies-boosters-based-on-antibody-levels [accessed May 2024].
Carlson C.J., Albery G.F., Merow C., Trisos C.H., Zipfel C.M., Eskew E.A., et al. 2022. Climate change increases cross-species viral transmission risk. Nature, 607: 555–562.
Carlson C.J., Gibb R.J., Albery G.F., Brierley L., Connor R.P., Dallas T.A., et al. 2022. The global virome in one network (VIRION): an atlas of vertebrate-virus associations. MBio, 13(2): e02985–e02921.
Castillo-Neyra R., Buttenheim A.M., Brown J., Ferrara J.F., Arvealo-Nieto C., Becerra V. et al. 2020. Behavioral and structural barriers to assessing human post-exposure prophylaxis and other preventive practices in Arequipa, Peru, during a canine rabies epidemic. PLOS Neglected Tropical Diseases, 14: e0008478.
Černe D., Hostnik P., Toplak I., Presetnik Pž, Maurer-Wernig J., Kuhar U. 2023 Discover of a novel bat lyssavireus in a long-fingered bat (Myotis capaccinii) from Slovenia. PLOS Neglected Tropical Diseases, 17(6): e0011420.
Chen R., Li H., Zhu W., Cheng H., Li Y., et al. 2024. Expert consensus on the clinical application of ormutivimab injection for use against the rabies virus. Expert Opinion on Drug Safety, 23(6): 755–762.
Coertse J., Grobler C.S., Sabeta C.T., Seamark E.C., Kearney T., et al. 2020. Lyssaviruses in insectivorous bats, South Africa, 2003–2018. Emerging Infectious Diseases, 26(12): 3056.
Coertse J., Viljoen N., Weyer J., Markotter W. 2023. Comparative neutralization activity of commercial rabies immunoglobulin against diverse lyssaviruses. Vaccines, 11(7): 1255.
Dato V.M., Campagnolo E.R., Long J., Rupprecht C.E. 2016. A systematic review of human bat rabies virus variant cases: evaluating unprotected physical contact with claws and teeth in support of accurate risk assessments. PLoS ONE, 11: e0159443.
de Paula Silva N., de Andrade EdA, Cardoso D., Guimarães R.C.S., Silva M.B., et al. 2021. Assessment of crab fishermen’s exposure to rabies virus in a typical Amazonian community. Zoonoses and Public Health, 68: 973–981.
Echevarría J.E., Banyard A.C., Mcelhinney L.M., Fooks A.R. 2019. Current rabies vaccines do not confer protective immunity against divergent lyssaviruses circulating in Europe. Viruses, 11: 892.
Endy T.P., Keiser P.B., Wang D., Jarman R.G., Cibula D., Fang H., et al. 2020. Serological response of 2 versus 3 doses and intradermal versus intramuscular administration of a licensed rabies vaccine for preexposure prophylaxis. The Journal of Infectious Diseases, 221(9): 1494–1498.
Fahrion A.S., Freuling C.M., Léchenne M., Müller T., Recuenco S., et al. 2023. Editorial: rabies, a long-standing one health example—progress, challenges, lessons and visions on the way to 0 by 30. Frontiers in Veterinary Science, 10: 1220327.
Fenton M.B., Rydell J. 2023. A miscellany of bats. Pelagic Press, London. 244p.
Fenton M.B., Simmons N.B. 2015. Bats: a world of science and mystery. University of Chicago Press, Chicago. 240p.
Fenton M.B., Jackson A.C., Faure P.A. 2020a. Bat rabies in Canada. In Taking the bite out of rabies: the evolution of rabies management in Canada. Edited by D. Gregory, R. Tinline, University of Toronto Press, Toronto. pp. 466–469.
Fenton M.B., Jackson A.C., Faure P.A. 2020b. Bat bites and rabies: the Canadian scene. Facets, 5: 367–380.
Fenton M.B., Mubareka S., Tsang S.M., Simmons N.B., Becker D.J. 2020c. COVID-19 and threats to bats. Facets, 5(1): 349–352.
Folly A.J., Marston D.A., Golding M., Shukla S., Wilkie R., Lean F.Z.X., et al. 2021. Incursion of European bat lyssavirus 1 (EBLV-1) in serotine bats in the United Kingdom. Viruses, 13: 1979.
Fooks A.R., Shipley R., Markotter W., Tordo N., Freuling C.M., Müller T., et al. 2021. Renewed public health threat from emerging lyssaviruses. Viruses, 13(9): 1769.
Frank E.G. 2024. The economic impacts of ecosystem disruptions: costs from substituting biological pest control. Science, 385(6713): eadg0344.
Franka R., Johnson N., Müller T., Vos A., Neubert A.L., et al. 2008. Susceptibility of North American big brown bats (Eptesicus fuscus) to infection with European bat lyssavirus type 1. Journal of General Virology, 89: 1998–2010.
Gan H., Hou X., Wang Y., Xu G., Huang Z., et al. 2023. Global burden of rabies in 204 countries and territories, from 1990 to 2019: results from the global burden of disease study. International Journal of Infectious Diseases, 126: 136–144.
D.J. Gregory, R.R. Tinline Editors. 2020. Taking the bite out of rabies: the evolution of rabies management in Canada. University of Toronto Press, Toronto. 672p.
Griffin D.R. 1958. Listening in the Dark. Yale University Press, New Haven. 413p.
Hamilton Medical Advisory. 2024. Medical advisory: human rabies case in Ontario. Available from https://www.hamilton.ca/city-council/news-notices/news-releases/medical-advisory-human-rabies-case-ontario.
Hanlon C.A., Kuzmin I.V., Blanton J.D., Weldon W.C., et al. 2005. Efficacy of rabies biologics against new lyssaviruses from Eurasia. Virus Research 111(1): 44–54.
Holzbauer S.M., Schrodt C.A., Prabhu R.M., Asch-Kendrick R.J., Ireland M., et al. 2023. Fatal human rabies infection with suspected host-mediated failure of post-exposure prophylaxis following a recognized zoonotic exposure—Minnesota. Clinical Infectious Diseases, 29: ciad098.
Irving A.T., Ahn M., Goh G., Anderson D.E., Wang L-Fa. 2021. Lessons from the host defenses of bats, a unique viral reservoir. Nature, 589: 363–370.
Jackson A.C., Fenton M.B. 2001. Human rabies and bat bites. The Lancet, 357: 1714.
Junior D.S.T., Marques M.S.V., Krummernauer A., Duarte M.M.S., Rocha S.M., et al. 2023. Rabies outbreak in Brazil: first case series in children from an indigenous village. Infectious Diseases of Poverty, 12: 78.
Kimitsuki K., Saito N., Yamada K., Park C.H., Inoue S., et al. 2020. Evaluation of the diagnostic accuracy of lateral flow devices as a tool to diagnose rabies in post-mortem animals. PLOS Neglected Tropical Diseases, 14: e0008844.
Klein A., Fahrion A., Finke S., Eyngor M., Novak S., et al. 2020. Further evidence of inadequate quality in lateral flow devices commercially offered for the diagnosis of rabies. Tropical Medicine and Infectious Disease, 5, 13
Klug B.J., Turmelle A.S., Ellison J.A., Baerwald E.F., Barclay R.M. 2011. Rabies prevalence in migratory tree-bats in Alberta and the influence of roosting ecology and sampling method on reported prevalence of rabies in bats. Journal of Wildlife Diseases, 47(1): 64–77.
Kuhn J.H., Adkins S., Alkhovsky S.V., Avšič-Županc T., Ayllón M.A., et al. 2022. Taxonomic update of phylum negarnaviricota (Riboviria: Orthornavirae), including the large orders Bunyavirales and Mononegavirales. Archives of Virology, 167: 2857–2906.
Kunkel A., Minhaj F.S., Pharm D., Whitehill F., Austin C., et al. 2022. Three human deaths attributed to bat exposures—United States, August 2021. MMWR Morbidity and Mortality Weekly Report, 71: 31–32.
T.H. Kunz, S. Parsons (Editors). 2009. Ecological and behavioral methods for the study of bats. 2nd ed. Johns Hopkins University Press, Baltimore. 920p.
Léchenne M., Naïssengar K., Lepelletier A., Alfaroukh I.O., Bourhy H., et al. 2016. Validation of a rapid rabies diagnostic tool for field surveillance in developing countries. PLOS Neglected Tropical Diseases, 10: e0005010.
Leon B., Gonzalez S.F., Solis L.M., Ramirez-Cardoce M., Moreir-Soto A., et al. 2021. Rabies in Costa Rica—next steps towards controlling bat-borne rabies after its elimination in dogs. The Yale Journal of Biology and Medicine, 94: 311–329.
Ma X., Bonaparte S., Corbett P., Orciari L.A., Gigante C.M., et al. 2023. Rabies surveillance in the United States during 2021. Journal of the American Veterinary Medical Association, 261: 1045–1053.
Mansfield K.L., Andrews N., Goharriz H., Goddard T., Mcelhinney L.M., Brown K.E., Fooks A.R. 2016. Rabies pre-exposure prophylaxis elicits long-lasting immunity in humans. Vaccine, 34: 5959–5967.
Markotter W., Coertse J. 2018. Bat lyssaviruses. Revue Scientifique et Technique de l'OIE, 37: 385–400.
Mauti S., Léchenne M., Naïssengar S., Traoré A., Kallo V., et al. 2020. Field postmortem rabies rapid immunochromatographic diagnostic test for resource-limited settings with further molecular applications. Journal of Visualized Experiments, (160).
Messenger S.L., Rupprecht C.E., Smith J.S. 2005. Bats, emerging virus infections, and the rabies paradigm. In Bat Ecology. Edited by T.H. Kunz, M.B. Fenton. University of Chicago Press, Chicago. pp. 622–679.
Moore S.M. 2021. Challenges of rabies serology: defining context of interpretation. Viruses, 2021; 13: 1516.
Moreno J.A., Baer G.M. 1980. Experimental rabies in the vampire bat. The American Journal of Tropical Medicine and Hygiene, 29: 254–259.
NACI (National Advisory Committee on Immunization). 2006. Rabies vaccine. Canada Immunization Guide (7th Edition, Part 4: Active Immunizing Agents, pp. 285–297). Public Health Agency of Canada, Minister of Public Works and Government Services Canada. Retrieved from Government of Canada Publications. Available from https://publications.gc.ca/collections/Collection/HP40-3-2006E.pdf [accessed October 2024].
Pancharoen C., Thisyakorn U., Tantawichien T., Jaijaroensup W., Khawplod P., Wilde H. 2001. Failure of pre- and postexposure rabies vaccinations in a child infected with HIV. Scand. J. Infect. Dis. 33: 390–391.
PHAC 2015. Part 4: Rabies vaccines. Canadian Immunization Guide (Internet). Ottawa, ON: Government of Canada; Publication update: 2015 January. Available from https://www.canada.ca/en/public-health/services/publications/healthy-living/canadian-immunization-guide-part-4-active-vaccines/page-18-rabies-vaccine.html#p4c17a6 [accessed October 2024].
Pieracci E.G., Pearson C.M., Wallace R.M., Blanton J.D., Whitehouse E.R., et al. 2019. Vital signs: trends in human rabies deaths and exposures—United States, 1938–2018. MMWR Morbidity and Mortality Weekly Report, 68(23): 524–528.
Racey P.A., Hutson A.M., Lina P.H.C. 2013. Bat rabies, public health and European bat conservation. Zoonoses and Public Health, 60: 58–68.
Rao A.K., Briggs D., Moore S.M., Whitehill F., Campos-Outcalt D., et al. 2022. Use of a modified preexposure prophylaxis vaccination schedule to prevent human rabies: recommendations of the Advisory Committee on Immunization Practices—United States. MMWR Morbidity and Mortality Weekly Report, 71: 619–627.
Simmons N.B., Cirranello A.L. 2024. Bat species of the world: a taxonomic and geographic database. Version 1.4. Available from https://batnames.org/ [accessed October 2024].
Stokstad E. 2017. Taming rabies. The best way to stop people from dying of rabies is to protect dogs. Science, 355: 238–242.
Stoner-Duncan B., Streicker D.G., Tedeschi C.M. 2014. Vampire bats and rabies: toward an ecological solution to a public health problem. PLoS Neglected Tropical Diseases, 8: e2867.
Tambe M.P., Parande M.A., Nanaware M.B., Salunke N.M., Dutta T., et al. 2024. Post-marketing surveillance of the world's first novel cocktail of rabies monoclonal antibodies: TwinRab™ in real-world setting. Indian Journal of Community Medicine, 49(2): 443–447.
Taylor L.H., Wallace R.M., Balaram D., Lidenmayer J.M., Eckery D.C., Mutonono-Watkiss B., et al. 2017. The role of dog population management in rabies elimination- a review of current approaches and future opportunities. Frontier in Veterinary Science, 2017, 4.
Tenzin T., Lhamo K., Rai P.B., Tshering D., Jamtsho P., et al. 2020. Evaluation of a rapid immunochromatographic test kit to the gold standard fluorescent antibody test for diagnosis of rabies in animals in Bhutan. BMC Veterinary Research, 16: 183.
Upham N.S., Esselstyn J.A., Jetz W. 2019. Inferring the mammal tree: species-level sets of phylogenies for questions in ecology, evolution and conservation. PLoS Biology, 17: e3000494.
Viljoen N., Weyer J., Coertse J., Markotter W. 2023. Evaluation of taxonomic characteristics of Matlo and Phala Bat rabies-related lyssaviruses identified in South Africa. Viruses, 15: 2047.
Walker P.J., Freitas-Astua J., Bejerman N., Blasdell K.R., Breyta R., et al. 2022. ICTV virus taxonomy profile: rhabdoviridae 2022. Journal of General Virology, 103, 001689.
Warren C.J., Sawyer S.L. 2023. Identifying animal viruses in humans: experimental virology can inform strategic monitoring for new viruses in humans. Science, 379: 982–983.
World Health Organization 2017. WHO Immunological basis for immunization series: module 17: rabies. Geneva, pp 1–49.
World Health Organization. 2018. Rabies vaccines: WHO position paper. Weekly Epidemiological Record, 93(16): 201–219.
Yale G., Gibson A.D., Mani R.S., PK H., Costa N.C., Corfmat J., et al. 2019. Evaluation of an immunochromatographic assay as a canine rabies surveillance tool in Goa, India. Viruses, 11(7): 649.
Appendix A. Always seek medical advice after a bat bite
The importance of PEP is illustrated by a case from Costa Rica (Leon et al. 2021) on 15 August 2018 when an unvaccinated 43-year-old high-school biology teacher was bitten by an insectivorous bat. He did not have PrEP and did not receive PEP. Two months later, he experienced pain, hyperesthesia, and paralysis of his arm and hand. A week later, he complained of fever, malaise, loss of appetite, nausea, vomiting, fluctuations in mental status, and paresis in his lower limbs. He was evaluated in a hospital emergency department where he was anxious, irritable, and confused, with mild sialorrhea, urine retention, and paralysis. He showed hemodynamic instability and neurological impairment requiring intubation and was admitted to an intensive care unit. Differential diagnoses included Guillain–Barre Syndrome and acute meningitis. After suspicion of rabies from the bite, samples of urine, saliva, cerebrospinal fluid, and a skin biopsy were sent to the laboratory. The skin biopsy tested positive for RABV nucleic acid by reverse transcription polymerase chain reaction (RT-PCR). The patient died on 14 November, a month after onset of illness. Postmortem, the positive RT-PCR product was sequenced, with 93.5% identity to RABV variants associated with the big brown bat, Eptesicus fuscus. Message: be careful handling bats, wear gloves, obtain PrEP, and always seek and receive PEP if bitten.
Appendix B. Carry proof of PrEP and latest titre
In January 2022, a bat biologist rescued three big brown bats (Eptesicus fuscus) from a building on a university campus. The biologist brought the bats home and fed and cared for them. Just before leaving for a field trip (February 2022), the bats were transferred to another researcher for release in the spring. A short time later, one of the bats showed clinical signs of encephalitic (furious) rabies. Previously, this bat had nipped the biologist and one canine tooth punctured their finger. The biologist had their RVNA checked before going to the field but did not carry the record of the titre result. After returning from field work, the biologist went to urgent care to report the bite. At urgent care they obtained the RVNA result of 6 IU/mL but insisted the biologist receive a PEP booster vaccine and a RIG administration. Fortunately, the biologist did not have an adverse reaction to the RIG and is fine and well today. Message: wear gloves, carry a copy of relevant RVNA results, and understand that RIG is only administered once to unvaccinated individuals.
Appendix C. Do not refuse PEP after contact with a known rabid animal. Seek post-PEP serological testing to ensure you are immunocompetent
On 27 July 2020 an 84-year-old man in Minnesota awoke with a bat biting his right hand. On 30 July 2020 RABV antigens were detected in the bat’s brain. Full PEP was initiated, including 20 IU/kg HRIG wound infiltration and four doses of vaccine. Exercising an abundance of caution, the patient’s wife received the same regimen. The patient died of rabies on 22 January 2021, and, together with the associated RABV variant based on the rabies variant, the biting bat was identified as a silver-haired bat, Lasionycteris noctivagans, based on 12S rRNA gene sequencing. This fatality was reported in the USA (Kunkel et al. 2022). Information in the press confused the situation, reporting that the incident in Minnesota occurred in Chicago and that the bat had bitten the man’s neck. Although it would seem that PEP failed in this case but this seems unlikely because of the short, 3-day delay to receive vaccine. Serological testing revealed that the patient was immunocompetent (Holzbauer et al. 2023). Message: knowing the species of bat and the variant of rabies virus was useful for epidemiological introspection but did not change the urgency of receiving PEP (including RIG). Post-PEP serological testing should be conducted to confirm an immunological response to rabies vaccine administration.
Appendix D.
Unfortunately, as this communication was going to press, local Canadian news outlets reported on a person hospitalized with a diagnosis of rabies, in an area where the primary author had worked in the field for many years. The suspected exposure was from a bat and occurred in the Gowganda area of the Timiskaming region, in northeastern Ontario. The case was confirmed by the Brant County Health Unit, located west of Hamilton, Ontario. This was the first case of human rabies reported in the Province in over 60 years (Hamilton Medical Advisory 2024). Message: if anyone has direct physical contact with a bat, even if there is no visible bite or scratch, or if they have been bitten or exposed to saliva or infected tissues from another animal species, they should contact their health care provider and/or report the incident to their local public health authority so they receive an immediate medical risk assessment, which usually means PEP and RIG.
Information & Authors
Information
Published In

FACETS
Volume 9 • Number 1 • January 2024
Pages: 1 - 11
Editor: Candace Nykiforuk
History
Received: 15 March 2024
Accepted: 29 June 2024
Version of record online: 8 November 2024
Copyright
© 2024 The Author(s). This work is licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Data Availability Statement
Not applicable.
Key Words
Sections
Subjects
Plain Language Summary
Preventing Exposure of Rabies from Bats to People
Authors
Author Contributions
Conceptualization: MBF, PAF, DJB, ACJ, TK, PHCL, WM, SMM, SM, PAR, CER, LW
Data curation: MBF, PAF, EB, DJB, PHCL, WM, SMM, SM, PAR, CER, LW
Formal analysis: MBF, PAF, EB, ACJ, PHCL, WM, SMM, PAR, CER
Investigation: MBF, PAF, EB, DJB, ACJ, TK, PHCL, SMM, PAR, CER
Resources: MBF, PAF, EB, DJB, PHCL, SMM, CER
Validation: MBF, PAF, EB, DJB, ACJ, TK, PHCL, WM, SMM, SM, PAR, CER, LW
Visualization: MBF, PAF, EB, DJB, ACJ, TK, PHCL, WM, SMM, PAR, CER, LW
Writing – original draft: MBF, DJB, SMM, PAR, CER
Writing – review & editing: MBF, PAF, EB, DJB, ACJ, TK, PHCL, WM, SMM, SM, PAR, CER, LW
Competing Interests
None.
Funding Information
DJB was supported by the USA National Science Foundation (NSF BII 2213854). PAF supported by the Natural Science and Engineering Research Council of Canada (NSERC RGPIN-2020-06906).
Metrics & Citations
Metrics
Other Metrics
Citations
Cite As
M. Brock Fenton, Paul A. Faure, Enrico Bernard, Daniel J. Becker, Alan C. Jackson, Tigga Kingston, Peter H.C. Lina, Wanda Markotter, Susan M. Moore, Samira Mubareka, Paul A. Racey, Charles E. Rupprecht, and Lisa Worledge. 2024. Bat handlers, bat bites, and rabies: vaccination and serological testing of humans at risk. FACETS.
9: 1-11.
https://doi.org/10.1139/facets-2024-0056
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
There are no citations for this item