Inventory and characteristics of Canadian interhospital transfer coordination structures
Abstract
Several studies have described interhospital transfer coordination structures in the US but there is a lack of data on Canadian coordination systems. We aimed to develop an inventory of existing interhospital coordinating structures across Canada and to detail how they operate in terms of governance, re-sources, tools, and processes. A cross-sectional survey was designed and ten managers/medical officials from seven coordination structures of interhospital transfers across Canada completed the survey. Findings indicate that coordination systems had similar communication modalities and covered similar services including the provision of medical advice. However, they differed in terms of the profile of staff processing transfers and transportation coordination. Mature structures such as Ontario and Alberta, who manage high annual volumes, distinguish themselves with very clear, standardized, and efficient processes, as well as implemented quality and performance improvement methods including key performance indicators. These results suggest that Canada may benefit from having an inter-provincial community of practice for interhospital transfer coordination structures to promote best practices, identify solutions, and harmonize services and processes. Better harmonization in transfer coordination would improve equity in the access to healthcare services. Future research should focus on the elaboration of evidence-and consensus-based guidelines that apply to the Canadian context.
Introduction
Interhospital patient transfers constitute an essential component of healthcare systems, allowing patients requiring transfer to access specialized services that are not available at their initial hospital. In addition, interhospital transfers can be used when the acute care capacity of a hospital is reached. In the case of patients requiring critical care, these transfers are often time critical and involve high-risk, unstable patients whose life depends on urgent intervention (Whiteley et al. 2011). While such a local and regional interhospital transfer strategy can prove effective for managing a localized disaster, it is ill-suited to deal with situations such as the COVID-19 pandemic in which the demand for acute care surges rapidly throughout an entire region (Anesi 2020).
The interregional transfer of patients was suggested as a measure to mitigate hospital bed shortfalls during the pandemic (Michelson et al. 2020; Myers and Nolan 2021; Sommer et al. 2022). In practice, implementing such a transfer strategy to cope with mounting cases throughout a region involved coordinating a large volume of interhospital transfers covering large geographic areas (CBC News 2021), which was a key strategy for outbreak preparedness. As a result, Canada and other countries implemented an interregional transfer strategy to manage rising demand for acute care (Reuters 2020; Tien et al. 2020; Guillon et al. 2021; Sanchez et al. 2021). Having up-to-date knowledge of where capacity beds were located and what kind of clinical services were offered in every critical care unit became essential to develop a judicious contingency plan for patients fighting COVID-19.
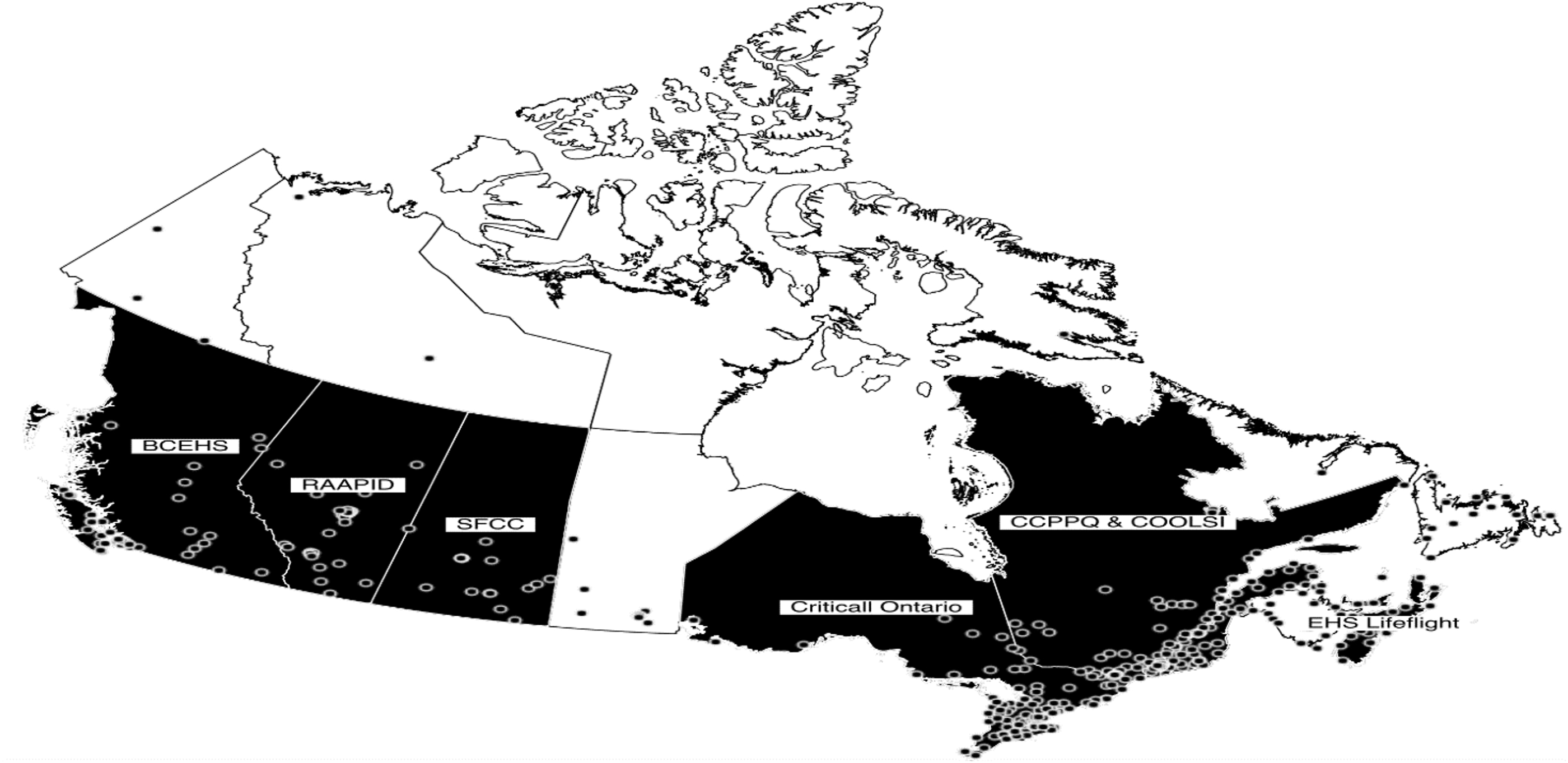
Fig. 1.
Systems to coordinate the interhospital transfer of patients can facilitate and expedite these transfers by determining patient needs, finding a suitable hospital department with the available capacity to receive the patient, and arranging the transfer between the referring and receiving hospitals. Yet, despite evidence of improved clinical outcomes in critical care trauma patients when their referrals are handled by a coordinating structure to reduce transfer delays (Evans et al. 2014; Moore et al. 2017, 2018), there is presently scant data on referral coordination systems in Canada, contrary to USA where several studies have described the regional coordination for specific trajectories such as trauma, ST elevation myocardial infarction, stroke (Health Service Executive 2014). Most of the literature related to interhospital transfer coordination structures deals with transport conditions (Eiding et al. 2019; Victoria Health and Human Services 2019) as such or on the impacts for patients (Eiding et al. 2019) or on transfer data (Kindermann et al. 2015). A large proportion of the structures identified are structures belonging to a hospital or a group of hospitals (Mayo Clinic 2016; Pagali et al. 2021) and having a system allowing real-time knowledge of the beds available is a fundamental aspect (Newton and Fralic 2015; Leroy et al. 2020) or even prior to a transfer coordination structure (Appui Santé and Médico-Social 2020).
In the Canadian context, little public information is available regarding their governance, resources, tools, and linkage with transportation coordination structures. Furthermore, to our knowledge, no critical care expert group or association has published official guidelines for the optimization of interhospital critical care transfers. A prerequisite to developing high-quality guidelines is to describe the structure of coordination systems. The overarching objective of the study was to draw up an inventory of interhospital transfer coordination systems in Canada (10 provinces and 3 territories). Specifically, we aimed to describe and compare Canadian coordination systems with regards to their governance, their resources, their tools, and their processes.
Methods
Study design, population, and socio-professional and demographic characteristics of respondents
Canadian coordinating structures were identified through queries to provincial health officials as well as discussions with hospital clinical staff regarding interhospital transfers. In total, seven structures were identified: British Columbia Emergency Health Services (BCEHS), Centre de Coordination en Périnatologie et Pédiatrie du Québec (CCPPQ), Centre d'Optimisation d'Occupation des Lits de Soins Intensifs (COOLSI), CritiCall Ontario, Emergency Health Services Lifeflight (EHS Lifeflight), Referral, Access, Advice, Placement, Information & Destination (RAAPID), and System Flow Coordination Centre (SFCC).
These coordination structures were identified in seven Canadian provinces out of ten, and in no Canadian territory. A total of 10 participants from these organizations took part in the survey among which nine were women (90%) and included two directors, an assistant to the director, two chiefs of service, a medical oversight physician, three managers, and a medical manager. They reported being in their current position for an average of 4.8 years (SD ± 3.9 years) and had previously occupied other positions within their organization. The average age of participants was 47.8 years (SD ± 7.9 years). All survey participants were required to provide informed consent in accordance with local regulations. The research did not require ethics committee approval.
Data collection
We targeted managers (medical, clinical, and/or administrative) of interhospital transfer coordination structures for recruitment. They were identified using provincial Ministry of Health websites, critical care program websites as well as through queries with the organizations.
Survey items were generated in accordance with published guidelines (Burns et al. 2008). First, a preliminary list of questionnaire items was generated following a strategic literature review on critical care interhospital transfers (Supplementary Material, Search Strategy). The list was then reviewed by experts in critical care to validate relevance and modify, remove, or add questions. A copy of the final survey is provided in Supplementary Material (Survey).
The survey was conducted, and results are reported in accordance with CROSS guidelines (Sharma et al. 2021). Participants were emailed an invitation containing a link to complete the survey on the Redcap platform (Harris et al. 2009) between April and December 2022. Non-responders were sent email reminders every 2 weeks up to four times after the initial invite. Participants were offered the option of completing the survey directly themselves or via a phone or video conferencing interview with a member of the research team. In addition, those who wanted to further elaborate on their survey responses could also request for a phone interview with a member of the research team to be scheduled. If needed, the research team also contacted respondents regarding any need for clarification on answers to questionnaire items or to resolve conflicting responses when they occurred.
Analyses
We opted for a descriptive approach to analyse the characteristics of the coordination structures. Certain results are explained in the text to underline the similarities and differences observed, while other results are presented in tables to show the presence or absence of certain elements.
Results
Description of coordinating structures and governance
A global presentation of the coordination structures (territory served, number of transfers requests processed annually, years existence number, composition of governance team, guidelines, and category of patients) is shown in Table 1. Canadian territories currently do not have coordination structures, which is an important result in itself.
Table 1.
| Coordinating structuresa | ||||||||
|---|---|---|---|---|---|---|---|---|
| BCEHS | CCPPQ | CRITICALL ONTARIO | COOLSI | EHS LIFEFLIGHT | RAAPIDb | SFCC | ||
| Territory servedc | British Columbia | Québec | Ontario | Québec | Nova Scotia and Prince Edward Island | Alberta | Saskatchewan | |
| Public or private | Public | Public | Public | Public | Private | Public | Public | |
| Number of transfers requests processed annually | 60 000 | 1400 | 48 000 | 9000d | 400e | 110 000 | 60 000 | |
| Years existence number (year) | >20 | 11–15 | >20 | 0–5 | 11–15 | 15–20 | 15–20 | |
| Composition of governance team | Manager | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Physician | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Nurses | ✓ | ✓f | ✓ | ✓ | ✓ | ✓ | ||
| Paramedics | ✓ | ✓ | ||||||
| Guidelines | On call physicians reachable at all times | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Mandatory use of the coordination team to transfer certain patients | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Life or limb policyg | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Implication of managers during medical conferences | ✓ | ✓ | ✓ | |||||
| Category of patients | Pediatric | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Adults | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
a
Although they are a part of their provincial health system, their involvement in the coordination of interhospital transfers grew out of their patient repatriation duties.
b
Although the use of the coordinating structure is not mandatory for interhospital transfers in Alberta, it was estimated by one of the respondents that 80%–90% of these transfers go through RAAPID.
c
Territory served concerns Canadian provinces. All structures except Alberta have a provincial government mandate. EHS Lifeflight responded that it covered two provinces (Prince Edward Island and Nova Scotia). It should be noted that three of the structures (BCEHS, RAAPID, and the SFCC) partitioned the province into two or more territories. For example, RAAPID partitioned Alberta into RAAPID north and RAAPID south. BCEHS operates three separated, but integrated, dispatch operations centers in Vancouver, Victoria, and Kamloops, which manage the receipt of all 911 calls and coordinate all responses to those calls. Further, RAAPID indicated that they handled transfer requests from eastern BC to Alberta hospitals and the BCEHS reported collaborating with other provinces and territories in the transfer of patients that are located near its borders. Although the question was not asked to respondents from other structures, similar arrangements regarding interhospital transfer to provide care to communities living close to interprovincial borders exist at CritiCall Ontario and the BCEHS. Similar arrangements may exist in other coordinating structures.
d
The respondent clarified that this number was closer to 1200 prior to COVID.
e
This number of requests processed annually (400) only concerns pediatric transfers.
f
Nurses have an educational role in the Critical Care Information System (CCIS) and not case facilitation.
g
The “life or limb policy” refers to a non-refusal policy for extreme urgent patients.
Regarding the roles of the governance team and the associated responsibilities, it was reported that the medical director in CritiCall Ontario is involved in out of country repatriation and participates at provincial tables while following up with provincial physicians if needed. There are also medical associates that are available in real time to resolve any conflicts or issues that require additional support to the call center. The executive director ensures the lead strategy, operating plan, and managing budgets.
At the CCPPQ, responsibilities of the governance team included training staff, the formalization of decisional algorithms, periodic reports, analysis of issues, quality improvement, escalation of problems to expert groups, or territorial medical managers, etc. There are managers who are responsible to manage systems and teams, to participate in provincial discussions and tables, while involved in strategy and operating plan.
At RAAPID, physicians act as a dyad with the manager/director to support clinical elements of the processes and engagement. Managers have a background in nursing and support day to day operations, change management and strategy.
Alike RAAPID, COOLSI co-management with a director and a medical manager is responsible for strategic development. Director is responsible for human resources.
EHS Lifeflight is a provincially paid, private company. Governance is by a president/COO (was a nurse), director with a large portfolio (was a nurse + paramedic), and senior manager (who was a paramedic). Their structure includes a medical director.
It was reported that the SFCC management included paramedics instead of nurses. Nurses help triage connections between physicians for patient transfers. Managers oversee the coordination centre.
At the BCEHS, there are no nurses in the governance team. Medical directors are responsible for health authorities (six different health authorities in British Columbia). Each department has a manager and a physician lead. The physician lead oversees any new initiative from a medical perspective and sits on board meetings that require a physician lead. They also have physicians on call 24/7 to help with prioritizing transfer and ground support for paramedics (approx. 44 physicians).
As for the guidelines in place (Table 1) and notably the mandatory use of the coordinating structure for the transfer of certain patients, BCEHS mentioned that all Life Limb and Threatened Organ patients or any patient that uses BCEHS resources should use the transfer coordination center in the eventuality of a transfer.
The CCPPQ indicated that it is mandatory for the transfer of at-risk pregnant women, newborns requiring intensive care and the reorientation of those under 18 years old requiring intensive pediatric care. The use of COOLSI is recommended for intensive care patients.
CritiCall Ontario indicated that it is mandatory for life-threatening or limb-threatening conditions. EHS Lifeflight reported that it was mandatory for transfer of neonatal and pediatric critical transfers. RAAPID answered that the PICU/NICU transfer teams were mandatory for neonatal and pediatric critical team transfers. The SFCC reported that it was mandatory in the transfer of trauma, critical and stroke cases.
Further, when asked if their coordination structure followed any other guidelines that were not listed among the options, the BCEHS reported that, with the exception of repatriations, the various subspecialties have their own specific guidelines developed by health authorities in collaboration with the BCEHS; COOLSI’s respondents reported resorting to the use of a coordinating physician when necessary. EHS Lifeflight reported triage amongst all services. RAAPID explained that they have specific call flows for different medical departments, to guide the regional placement of patient.
Resources
Table 2 describes the communication channels used to make a transfer request.
Table 2.
| Resources | Coordinating structure | |||||||
|---|---|---|---|---|---|---|---|---|
| BCEHS | CCPPQ | CRITICALL ONTARIO | COOLSI | EHS Lifeflight | RAAPID | SFCC | ||
| British Columbia | Quebec pediatric | Ontario | Quebec adult | Nova Scotia and Prince Edward Island | Alberta | Saskatchewan | ||
| Communication channels | Call center | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Computer systems for the transfer of medical images | ✓ | ✓ | ✓ | |||||
| Web system | ✓ | ✓ | ||||||
| Fax | ✓ | |||||||
| Profile of the employees | Nurse | ✓ | ✓ | ✓ | ✓ | |||
| Administrative support staff | ✓ | ✓ | ✓ | ✓ | ||||
| Physicians | ✓ | ✓ | ||||||
Tools
All coordinating structures except EHS Lifeflight use dashboards to assist in coordinating interhospital requests (Table 3). Concerning additional information displayed on the dashboard, the BCEHS mentioned pending requests and their status and CritiCall Ontario reported information regarding distances and special considerations. All the dashboards had restricted access to main users and not public access to all the healthcare network. The other tools used by the coordinating structures are shown inTable 3.
Table 3.
| Tools | Coordinating structure | |||||||
|---|---|---|---|---|---|---|---|---|
| BCEHS | CCPPQ | CRITICALL ONTARIO | COOLSI | EHS Lifeflight | RAAPID | SFCC | ||
| British Columbia | Quebec Pediatric | Ontario | Quebec Adult | Nova Scotia and Prince Edward Island | Alberta | Saskatchewan | ||
| Data displayed on the dashboard | Beds available per hospital | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Specialized services offered at each hospital | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| Data on interhospital transport | ✓ | ✓ | ||||||
| Clinical information on the reasons for occupation of intensive care beds | ✓ | ✓ | ||||||
| Repertory of specialized hospital resources | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| aScripts for call centre operators | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Checklist | ✓ | ✓ | ✓ | ✓ | ||||
| Clinical/administrative Algorithms | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ||
| Computer system allowing data collection of transfer coordination | ✓ | ✓ | ✓ | ✓ | ✓ | |||
| Other | bvideo conferencing tool | Record system Komlog | ||||||
a
Scripts for call center operators refer to questions that they have to ask, while clinical or administrative algorithms refer to swimlane diagrams or other forms of documents detailing the process in its entirety, to standardise the transfer process.
b
bConcerning video conferencing tools used by BCEHS, there are MOCAP to know physician on call scheduled for all hospitals and PROMAP where all processes and guidelines and policies are housed to guide workers.
Processes
Regarding the services offered (Table 4) for medical advice/tele expertise, it is provided by physicians from the structure at EHS Lifeflight, by physicians from the territory in five structures (BCEHS, CCPPQ, CritiCall Ontario, RAAPID, and SFCC) and by a physician from either the territory or from the structure in one case (COOLSI). Among the six structures that handled patient repatriation requests, the coordination of these transfers could be processed by clinical staff only in four (CCPPQ, COOLSI, EHS Lifeflight, SFCC), by nonclinical or clinical staff in RAAPID, by nonclinical staff in BCEHS. All structures except for COOLSI offered a certain level of specialized interhospital transport coordination.
Table 4.
| Services | Coordinating structures | ||||||
|---|---|---|---|---|---|---|---|
| BCEHS | CCPPQ | CRITICALL ONTARIO | COOLSI | EHS Lifeflight | RAAPID | SFCC | |
| British Columbia | Quebec Pediatric | Ontario | Quebec adult | Nova Scotia and Prince Edward Island | Alberta | Saskatchewan | |
| Urgent transfers | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| Semi-urgent transfers | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Non-urgent transfers | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Patient repatriation | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Coordination of requests for medical opinion/tele-expertise | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ |
| aManagement of exceptional health situations | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
| Specialized interhospital transport | ✓ | ✓ | ✓ | ✓ | ✓ | ✓ | |
a
Example of Covid-19 pandemic or a Code Orange that is used to respond safely and effectively to a disaster external to the hospital that is likely to increase the capacity and use of hospital resources.
Table A in Supplementary Material shows for which care units the various coordinating structures processed transfer requests. When asked if they performed interhospital transfer coordination for any other units, the BCEHS specified that it regularly handled transfer requests for all units except rehabilitation. The CCPPQ reported that it handled requests for the perinatology and pediatric units. RAAPID also could process urgent transfer requests from clinics and COOLSI reported that it took on psychiatry and rehabilitation center transfer requests only to face the pandemic situation. BCEHS elaborated that transfer requests were either classified as red, which were processed as soon as possible, yellow, in which the time was specified by admitting specialist, green, which were scheduled appointments, so the targets were to make their appointment or blue, which were patient repatriations for which there were no target; CritiCall reported that it had two priorities: life or limb, where the target was 10 min or urgent and emergent where the associated delay was 15 min. All structures except the CCPPQ and CritiCall Ontario had a process in place for the transfer of patients from specialized to less specialized services.
Three structures, the BCEHS, CritiCall Ontario, and RAAPID arrange transportation once the destination had been identified and the remainder does not. These structures that make transportation arrangements do so for ground, airplane, or helicopter transportation. Only the BCEHS has its own transport team, the other two working with external partners.
Regarding the type of information asked and collected during the transfer, it was reported that all structures collected information on the reason for transfer. Every structure except CritiCall Ontario collected information on patient vital signs. Every structure except for the BCEHS and CritiCall Ontario collected information on patients summary of hospital courses. The CCPPQ and EHS Lifeflight reported collecting information on medication lists. The CCPPQ and EHS Lifeflight also collected information on lab reports. It was also reported that BCEHS, COOLSI, and EHS Lifeflight collected radiological images during transfers.
Finally, when asked if any other information was asked during the transfer, the BCEHS reports that depending on the transfer, it collects information on infectious precautions, if there was trauma (if relevant), whether the patient is intubated or not. The CCPPQ responded that the COVID test results were asked; RAAPID also collected information on care needs, that is, need for isolation, transport needs, and safety concerns.
The modalities used for sharing clinical information are detailed in Table B (Supplementary Material) and those relating to the updates between transfer acceptance and patient transport are displayed in Table C (Supplementary Material).
We also inquired about the performance indicators for which the results are displayed in Table D in Supplementary Material. As for additional performance indicators used within their organization, the CCPPQ mentioned the number of transfers to measure performance; COOLSI indicated time to acceptance; CritiCall Ontario quoted time to first call out, time to patient acceptance, time of arrival, whether the patient is declared life or limb or not and whether the consultation was accepted or declined with the associated reason. Finally, the BCEHS reported calls in waiting/answered to determine if their services are meeting the level of demand. The measures in place to ensure continuous improvements are presented in Table E in Supplementary Material.
All but one of the structures (EHS Lifeflight) were reported to have changed their processes due to the COVID-19 pandemic. At the CCPPQ, the changes were the existence of COVID-19 designated centers, the implementation with COOLSI of an algorithm to organize who does what as well as in which context to call the COOLSI and higher accountability. At the COOLSI, the pandemic resulted in added responsibilities, as it also took on transfer toward regular wards, as well as rehabilitation and psychiatry patients, in addition to ministerial instructions regarding dedicated COVID centers and changes in capacity. CritiCall Ontario reported that they needed to stay on top of changes and processes as the need arose: they were at the Covid Command Table and involved in discussions, policy changes, and changes to level of authority for movement of patients. CritiCall Ontario was also involved with Saskatchewan and Manitoba in moving patients to Ontario and back to their provinces. In addition, CritiCall Ontario continued to support the re-opening and sustainability of the system and worked to finalize the redirect process for hospitals and regions. Finally, CritiCall Ontario was actively involved in several projects to further assist with rural needs and virtual care opportunities. RAAPID reported that more requests became coordinated within their structure, which was not mandatory, to improve communication and predictability of patient movement between sites, particularly those with COVID symptoms. Consequently, there was involvement of their team with increased frequency in more movements. The SFCC went from being a regional coordination structure to a provincial one.
Discussion
Survey results highlighted some similarities (Supplementary Material, IMAGE A). We found that all structures manage interhospital transfers for some specialized trajectories. This finding is consistent with other researches realised in the USA which mention the existence of structured regional coordination only for specific pathways like trauma, ST myocardial infarction, and cerebrovascular accident (Feazel et al. 2015; Kindermann et al. 2015).
Our results also show that all interhospital transfer coordination structures have a call center as the main entrance point. They follow the scripts for their interventions and most of them use algorithms to standardize the transfer process. Previous studies about coordination centers performance (Pagali et al. 2021) as well as articles published about the Mayo Clinic (Mayo Clinic 2016) experience in Minnesota have indicated that electronic algorithms help determine the specialized service and appropriate level of care.
However, our study also revealed a large heterogeneity of the systems that could compromise their efficacy and effectiveness. The fact that healthcare is a provincial jurisdiction in Canada could explain this heterogeneity. Most structures seem to be bottom-up initiatives that are aimed to answer time-dependent clinical conditions and day to day pitfalls that clinicians were facing while having to organize interhospital transfers. Recent publications (Grier et al. 2020; NHS. Adult Critical Care Transfer service specification 2021) in England show that there is considerable variability among the regions, but the creation of “Adult Critical Care Transfer Services” by the National Health Service (NHS) should fill this role. In France, the «Services d'Aide Médicale Urgente-SAMU» are in charge of interhospital transfers (Leroy et al. 2020), but according to a 2020 report (Appui Santé and Médico-Social 2020) there is no territorial organization. In Norway, according to a 2019 article (Eiding et al. 2019), the responsibility to organize transfers belongs to hospitals. Our results also indicate differences in the type of information displayed on the dashboard and performance indicators. Interhospital transport management alternates between the absence of coordination, reliance on own transport team, or reliance on external partners. Although interhospital transport is still organized for any of the situations mentioned above, available studies (Newton and Fralic 2015) show that colocation of the transportation team with those coordinating available beds and those of the call center facilitates collaboration and speeds up transfers.
Almost all the structures have reported that the COVID-19 pandemic has brought organizational, technical, and human changes in the management of the interhospital transfers. Literature on the COVID-19 crisis has highlighted the weaknesses of information systems and structures for the coordination of interhospital transfers experiences to be learned from going forward. As a response to COVID-19 in USA, Centers for Disease Control and Prevention have encouraged the creation of a «Regional Medical Operations Coordinating Cell-MOCC» in every state (Centers for Disease Control and Prevention 2020).
Strengths of this study include the collection of data. We conducted this study according to Canadian healthcare professional survey recommendations and reported results according to the CONSORT checklist, CROSS. However, this research does have limitations. We were unable to collect information on three provinces (Manitoba, New Brunswick, and Newfoundland and Labrador) or any of the Canadian territories. We only identified one or two respondents from each province so responses may be subject to misclassification due to differing perceptions or understanding of questions. Lastly, our questionnaire was based on a rapid review of the literature and may therefore not represent an exhaustive portrait of all-important elements of a system.
This study represents an important advancement in knowledge on interhospital transfer coordination systems in Canada, with a focus on governance, process, and tools. This knowledge could serve as a foundation for the elaboration of guidelines for efficient coordination transfer structures. In this regard, Canada would benefit from improving existing coordination models in different ways. For example, ensuring that each territory has a single point of contact would help reduce delays and improve patients’ clinical progress. The single point of contact should cover all patients’ needs, whether the specialty or subspecialty. In addition, it should have control over the resources required for patient transfer, which includes land and air transportation. This will greatly benefit the clinicians and result in significant time savings. While the current point of contact is mainly by telephone, the latter should migrate to a computerized format linked to existing systems. Such information systems would, especially, speed up data collection and improve its reliability by integrating decision-making algorithms. Therefore, human resources could be used more appropriately, where clinical and human judgment is required. Note that, electronic computerized systems also open doors to the potential contributions of learning algorithms and artificial intelligence.
Finally, for equitable access to care and services for all patients, provincial authorities should align with each other for possible interprovincial transfers and to process international repatriations. In fact, the heterogeneity of existing models we observed raises concern about the variations in both access to and the provision of healthcare across Canada. Furthermore, the absence of these structures in certain provinces or territories raises concern about equity in our country. Further research is needed that would focus on the following aspects: evaluate the impact of differences in structures on clinical outcomes and resource use to identify optimal structural elements.
Acknowledgements
This research was funded by the Réseau Québécois COVID-Pandémie. We also wish to thank Stephane Ahern and Abel Vanderschuren for their feedback during survey development. We also wish to thank study participants for the time they gave to this project.
References
Anesi G.L. 2020. Hospital transfers across U.S. regions to address the «space» shortage in a pandemic: a public good. Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America. ciaa1596.
Appui Santé & Médico-Social. 2020. Premiers éléments d'organisation des filières de soins critiques en France. Available from https://www.preventioninfection.fr/wp-content/uploads/2020/06/2020_Elements-Org-Filieres-Soins-critiques_ANAP.pdf [accessed November 22, 2024].
Burns K.E.A., Duffett M., Kho M.E., Meade M.O., Adhikari N.K.J., Sinuff T., Cook D.J. 2008. A guide for the design and conduct of self-administered surveys of clinicians. Canadian Medical Association Journal, 179(3): 245.
CBC News. (2021, avril 21). Ontario hospitals hit by COVID-19 transferring record number of patients around province | CBC News. CBC. Available from https://www.cbc.ca/news/canada/toronto/ontario-hospitals-patient-transfers-unprecedented-number-covid-19-pandemic-1.5995499 [accessed November 22, 2024].
Centers for Disease Control and Prevention. 2020. Key considerations for transferring patients to relief healthcare facilities when responding to community transmission of COVID-19 in the United States. Available from https://www.cdc.gov/coronavirus/2019-ncov/hcp/relief-healthcare-facilities.html [accessed November 22, 2024].
Eiding H., Kongsgaard U.E., Braarud AC. 2019. Interhospital transport of critically ill patients: experiences and challenges, a qualitative study. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine, 27(1): 27.
Emergency Health Services Lifeflight, https://ehslifeflight.ca/
Evans C.C.D., Tallon J.M., Bridge J., Nathens A.B. 2014. An inventory of Canadian trauma systems : opportunities for improving access to trauma care. CJEM, 16(3): 207‑213.
Feazel L., Schlichting A.B., Bell G.R., Shane D.M., Ahmed A., Faine B., et al. 2015. Achieving regionalization through rural interhospital transfer. American Journal of Emergency Medicine, 33(9):1288–1296.
Grier S., Brant G., Gould T.H., von Vopelius-Feldt J., Thompson J. 2020. Critical care transfer in an English critical care network: analysis of 1124 transfers delivered by an ad-hoc system. Journal of the Intensive Care Society, 21(1):33–39.
Guillon A., Laurent E., Godillon L., Kimmoun A., Grammatico-Guillon L. 2021. Inter-regional transfers for pandemic surges were associated with reduced mortality rates. Intensive Care Medicine, 47(7): 798‑800. PubMed.
Harris P.A., Taylor R., Thielke R., Payne J., Gonzalez N., Conde J.G. 2009. Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics, 42(2): 377‑381.
Health Service Executive. 2014. “Right Care, Right Now”: model of care for adult critical care—National Clinical Programme for Critical Care. Available from https://www.hse.ie/eng/services/publications/clinical-strategy-and-programmes/model-of-care-for-adult-critical-care.pdf [accessed November 22, 2024].
Kindermann D.R., Mutter R.L., Houchens R.L., Barrett M.L., Pines JM. 2015. Emergency department transfers and transfer relationships in United States hospitals. Academic Emergency Medicine, 22(2):157–165.
Leroy C., Treluyer L., Hellmann R., Cléry R., Haab F., Parc Y. 2020. Retour d'expérience sur la cellule régionale d'appui à la régulation des lits de réanimation Covidréa pendant la crise Covid-19. Annales françaises de médecine d'urgence, 10(4-5):321–326.
Mayo Clinic. 2016. ATC, ECC expedite transfers, support referring providers. Available from https://www.mayoclinic.org/medical-professionals/trauma/news/atc-ecc-expedite-transfers-support-referring-providers/mac-20429458 [accessed November 22, 2024].
Myers V., Nolan B. 2021. Delays to initiate interfacility transfer for patients transported by a critical care transport organization. Air Medical Journal, 40(6): 436–440.
Michelson K.A., Rees C.A., Sarathy J., VonAchen P., Wornow M., Monuteaux M.C., Neuman M.I. 2020. Interregional transfers for pandemic surges. Clinical Infectious Diseases. ciaa1549.
Moore L., Champion H., Tardif P.-A., Kuimi B.-L., O'Reilly G., Leppaniemi A., et al. 2018. Impact of trauma system structure on injury outcomes : a systematic review and meta-analysis. World Journal of Surgery, 42(5): 1327‑1339.
Moore L., Evans D., Hameed S.M., Yanchar N.L., Stelfox H.T., Simons R., et al. 2017. Mortality in Canadian trauma systems : a multicenter cohort study. Annals of Surgery, 265(1): 212‑217.
Newton S.M., Fralic M. 2015. Interhospital transfer center model: components, themes, and design elements. Air Medical Journal, 34(4):207–212.
NHS. 2021. Adult critical care transfer service specification. Available from https://www.england.nhs.uk/wp-content/uploads/2021/06/Adult-critical-care-transfer-service-specification-2023-v0.6-FINAL.pdf [accessed November 22, 2024].
Pagali S., Kocher J.P., Coons T., King K., Hansel S., Van Brunt N., et al. 2021. Quality performance of a transfer center reduces interhospital transfer and direct admission-related ED evaluations. American Journal of Medical Quality, 12:12.
Reuters. 2020. EU to fund transfer of COVID-19 patients across borders to prevent hospital collapse. Reuters. Available from https://www.reuters.com/article/us-health-coronavirus-eu-overwhelmed-idUSKBN27E3K3 [accessed November 22, 2024].
Sanchez M.-A., Vuagnat A., Grimaud O., Leray E., Philippe J.-M., Lescure F.-X., et al. 2021. Impact of ICU transfers on the mortality rate of patients with COVID-19 : Insights from comprehensive national database in France. Annals of Intensive Care, 11(1): 151.
Sharma A., Minh Duc N.T., Luu Lam Thang T., Nam N.H., Ng S.J., Abbas K.S., et al. 2021. A consensus-based checklist for reporting of survey studies (CROSS). Journal of General Internal Medicine, 36(10): 3179–3187.
Sommer A., Rehbock C., Vos C., Borgs C., Chevalier S., Doreleijers S., et al. 2022. Impacts and lessons learned of the first three COVID-19 waves on cross-border collaboration in the field of emergency medical services and interhospital transports in the Euregio-Meuse-Rhine : a qualitative review of expert opinions. Frontiers in Public Health. 10.
Tien H., Sawadsky B., Lewell M., Peddle M., Durham W. 2020. Critical care transport in the time of COVID-19. Canadian Journal of Emergency Medicine, 22(S2): S84–S88.
Victoria Health and Human Services. 2019. Time critical defined transfer guidelines. Available from https://www.ambulance.vic.gov.au/wp-content/uploads/2016/03/time-critical-defined-transfer-guideline.pdf [accessed November 22, 2024].
Whiteley S., Macartney I., Mark J., Barratt H., Binks R. 2011. Guidelines for the transport of the critically ill adult.
Supplementary material
Supplementary Material 1 (DOCX / 14 KB).
- Download
- 13.17 KB
Supplementary Material 2 (DOCX / 421 KB).
- Download
- 420.31 KB
Information & Authors
Information
Published In

FACETS
Volume 10 • 2025
Pages: 1 - 8
Editor: Candace Nykiforuk
History
Received: 23 November 2023
Accepted: 14 September 2024
Version of record online: 27 January 2025
Copyright
© 2025 The Authors. This work is licensed under a Creative Commons Attribution 4.0 International License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Data Availability Statement
All relevant data are within the paper and in the Supplementary Material.
Key Words
Sections
Subjects
Plain Language Summary
Overview of Canadian systems for hospital transfers
Authors
Author Contributions
Conceptualization: MD, CO
Formal analysis: MD, DN, AAK
Funding acquisition: MD, CO
Investigation: DN, AAK
Methodology: LM
Supervision: MD, CO
Visualization: AAK, DB
Writing – original draft: MD, DN, CO
Writing – review & editing: MD, LM, DN, AAK, DB, CO
Competing Interests
The authors have declared that no competing interests exist.
Funding Information
Réseau Québécois COVID-Pandémie
Metrics & Citations
Metrics
Other Metrics
Citations
Cite As
Marie-Eve Desrosiers, Lynne Moore, David Nguyen-Tri, Aubin Armand Keundo, Denis Boutin, and Caroline Ouellet. 2025. Inventory and characteristics of Canadian interhospital transfer coordination structures. FACETS.
10: 1-8.
https://doi.org/10.1139/facets-2023-0209
Export Citations
If you have the appropriate software installed, you can download article citation data to the citation manager of your choice. Simply select your manager software from the list below and click Download.
There are no citations for this item